
Please enable JavaScript to use all features of this page.
Synopsis of Sinus of Valsalva Aneurysm (SOVA)
Synopsis
Definition
A weakness of the aortic wall that leads to focal bulging, aneurysm formation or windsock deformity.
Gender and Prevalence
- Male:Female 4:1
- Western population 0.14 – 0.23%
- Asian population 0.46 – 3.5%
Etiology
- Congenital – Majority of cases and usually affects single sinus only.
- Acquired – Less common. Acquired defects occur secondary to conditions which affect the aortic wall leading to degeneration of the elastic and connective tissue elements. This often results in diffuse dilatation of all 3 sinuses which contrasts to the single isolated sinus lesion seen among congenital patients. Associated conditions include:
- Syphilis
- Trauma
- Endocarditis
- Atherosclerosis
- Marfans (diffuse dilatation)
- Uncommon – Ehlers Danlos (other connective tissue disorders), Takayasu arteritis (other vasculitides), post AV replacement
Pathophysiology
- Congenital SOVA results from a developmental defect of the bulbar cordis causing a discontinuity and lack of elastin between the media of the aortic sinus and hinge line of the aortic annulus.
- Acquired SOVA occurs due to aortic wall degeneration of elastin and connective tissue elements.
- In both conditions, prolonged exposure to high aortic pressures leads to aneurysm formation.
Site
Associated Anomalies
- VSD (30-60%) - supracristal (majority) or perimembranous
- Bicuspid AV (15-20%)
- Aortic insufficiency (40-50%) from cusp prolapse (usually RCC with VSD)
- Other - Pulmonary stenosis (usually subvalvular), coarctation of the aorta, PDA, ASD
Asian series demonstrate a higher incidence of right SOVA which more commonly rupture into the RV, higher incidence of VSD and lower incidence of bicuspid AV compared to Western populations.
Clinical Presentation
- Unruptured - Largely asymptomatic. Occasionally present with arrhythmias (CHB, AF, VT) from compression of atrioventricular node (AVN), IVS and bundle of His or myocardial ischemia from obstruction of coronary blood flow (CBF).
- Ruptured - There are 3 patient groups defined based on size of ruptured orifice, rapidity of rupture and which chamber the rupture has occurred into
- 35% acute symptoms (dyspnea, chest pain)
- 45% gradual dyspnea
- 20% asymptomatic and diagnosed with a new murmur
Indicators for Surgical Intervention
- Rupture (fig. 3a, 3b, 3c)
- Endocarditis
- Unruptured large or complex SOVA – Controversial. Generally, repair recommended if:
- Complications of VSD, AI, RVOT obstruction, MR, arrhythmias and infection
- Large SOVA which have high potential for late complications of myocardial ischemia and rupture
- Unruptured, small and asymptomatic SOVA – No clear guidelines but serial echo evaluation advisable
{kind=link}
{kind=link}
{kind=link}
Surgical Options
- For congenital SOVA, windsock excision, closure of SOVA defect, and if needed VSD patch repair, closure of fistula and aortic valve repair.
- Aortic valve replacement maybe required in patients with calcified bicuspid AV or moderate-severe AI causing cusp retraction, thickening and calcification.
- Root replacement or Ross procedure maybe used if severe local septic etiology.
Complications
- Rupture into RV > RA > LV > IVS/PA leads to formation intracardiac fistulae or tamponade. Congenital SOVA most commonly rupture between 15 – 30 years either spontaneously or secondary to strenuous physical activity, trauma or endocarditis.
- Myocardial ischemia from decreasing CBF or coronary thrombosis
- Endocarditis
- Sudden death from arrhythmia or left main coronary artery compression
Survival
10 year survival post-surgical repair 94%
Figures & Videos
- Fig. 1a Colour compare midesophageal AV LAX view depicting rupture of a right Sinus of Valsalva aneurysm into the right ventricle with an associated subaortic ventricular septal defect.
- Fig. 1b Colour compare midesophageal AV SAX view of a rightSinus of Valsalva aneurysm showing flow into the right ventricle.
- Fig. 2a Colour compare 2D midesophageal AV SAX depicting rupture of non-coronary Sinus of Valsalva aneurysm into the right atrium with unidirectional turbulent flow.
- Fig. 2b 3D full volume of the AV SAX displaying a non-coronary Sinus of Valsalva aneurysm. Drop out at tip of windsock is an echo feature consistent with rupture.
- Fig. 2c 3D colour Doppler demonstrating a ruptured non-coronary SOVA windsock to right atrial fistula with unidirectional turbulent flow.
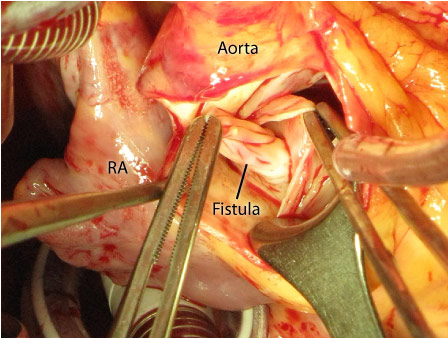
- Fig. 3a Non-Coronary sinus – Right atrial fistula pulled inside-out into the aorta.
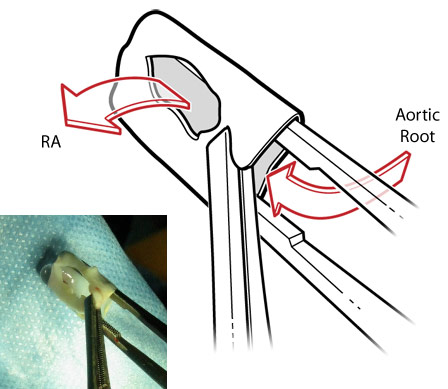
- Fig. 3b Ruptured non-coronary Sinus of Valsalva aneurysm. Arrows depict direction of blood flow through the defect between the aorta and right atrium.
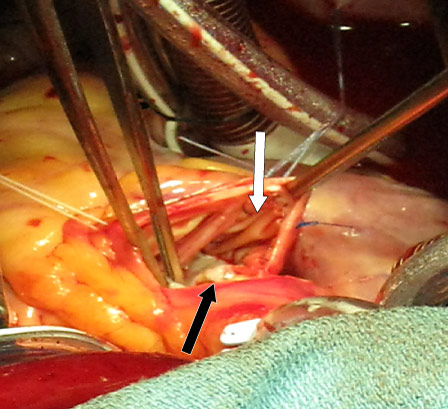
- Fig. 3c Excision of fistula and aneurysm with pericardial patching of the non-coronary sinus. Non-Coronary Cusp (black arrow). Non-Coronary Sinus bovine pericardial patch (white arrow).
- Fig. 4 Colour compare 2D midesophageal 5Ch demonstrating the midesophageal five chamber view of a non-coronary SOVA.
- Fig. 5a 2D midesophageal AV SAX demonstrating a windsock deformity of non-coronary SOVA.
- Fig. 5b Full volume 3D demonstrating a windsock deformity of non-coronary SOVA.
- Fig. 6a 2D midesophageal AV SAX demonstrating a ruptured left Sinus of Valsalva aneurysm with surrounding thrombus.
- Fig. 6b 2D colour midesophageal AV SAX demonstrating a ruptured left Sinus of Valsalva aneurysm with surrounding thrombus.
- Fig. 7a 2D midesophageal 4Ch demonstrating a moderately dilated right ventricle.
- Fig. 7b 3D midesophageal 4Ch demonstrating a moderately dilated right ventricle.
Echo Features
TEE views used for diagnosis
What to look for in 2D and 3D TEE
- Sinus dilatation
- Single (congenital) or mutiple (acquired) sinus involvement
- SOVA location + measure size
- Identify cardiac chamber which SOVA expands into
- Identify presence of windsock deformity of the SOVA which expands during systole (fig. 5a, 5b)
- Echo dropout at tip of the windsock may indicate rupture7(fig. 2b)
- Sinus thrombus (fig. 6a, 6b)
- RV/LV volume overload /dilatation (fig. 7a, 7b)
- RV/LV systolic function
What to look for in Colour Doppler
- Presence of ruptured versus unruptured SOVA
- Flow is typically turbulent or laminar in thrombosed and low flow state
- Identify location of rupture and fistula formation
- Determine shunt direction
What to look for in Spectral Doppler
- Determine peak/mean pressure gradients across intracardiac fistulae
- Determine the timing and duration of fistula flow with reference to the ECG
- Aortic-intracardiac fistula demonstrates continuous systolic + diastolic high velocity unidirectional flow
- VSD demonstrates high velocity systolic + low velocity diastolic flow
- If both conditions are present, continuous high velocity aortic-intracardiac fistula flow may mask the VSD Doppler spectrum7
Associated Conditions
VSD
Views
- ME 5 Ch
- ME 4 Ch
- ME AV LAX
- ME RV in/outflow
- TG SAX/LAX
- Deep TG LAX
2D/3D
- Location + size of defect
- Type (subarterial/supracristal > perimembranous)
Colour Doppler
- Subarterial – Colour flow sub-pulmonic (RV in/outflow)
- Perimembranous – Colour flow subtricuspid within anterior IVS (RV in/outflow, TG SAX)
Spectral Doppler
- Peak/mean pressure gradients
- Restrictive Vs unrestrictive
- High velocity systolic L to R flow
BAV/Aortopathy
Views
- ME AV SAX/LAX
- ME AscAo SAX/LAX
- UE AoArch SAX/LAX
2D/3D
- Bicuspid/Tricuspid Valve
- Cusp Prolapse
- Aortic Regurgitation
- Aortopathy (dilated or aneurysmal +/-dissection)
- Aortic dimensions
- Repair unlikely if thickened, rolled, and calcified cusps
Colour Doppler
- Colour flow across AV to assess severity AR
- Eccentric jet (cusp prolapse) Vs central (root dilatation)
Spectral Doppler
- AV Peak/mean pressure gradients, AV VTI
- AR, PHT/Deceleration time
Endocarditis
2D/3D
- Valvular mobile mass associated with SOVA.
- Assess other valves for vegetations
- Assess for valve perforation, local abscess and fistulae formation
Colour Doppler
- Valve regurgitation/stenosis
- Multiple jets in valve perforation
- Abscess with fistuale show complex intracardiac communications
RVOT Obstruction/Pulmonary valve stenosis
Views
- UE AoArch SAX
- ME AscAo SAX
- ME RV in/outflow
- TG RV in/outflow
2D/3D
- Prolapse RCC
- Pulmonary valve morphology, mobility
- Sub-pulmonic valve narrowing/shelf
- Post stenotic dilatation of pulmonary artery
Colour Doppler
- Pulmonary stenosis (systolic turbulence post PV)
- Subpulmonic stenosis (systolic turbulence RVOT)
- Pulmonary regurgitation
Spectral Doppler
- PV Peak/mean pressure gradient
- Subpulmonic obstruction gives dagger shaped CW Doppler
Other Related Anomalies
- ASD
- PDA
- Coarctation of the aorta
- Gerbode effect (shunt LV to RA)
References
- Wang ZJ et al. Surgical repair of sinus of Valsalva aneurysm in asian patients. Ann Thorac Surg 2007;84:156-60
- Ring S. Congenital heart surgery nomenclature and database project; aortic aneurysm sinus of valsalva aneurysm and aortic dissection. Ann Thorac Surg 2000;69:S147-63
- Yan F et al. Surgery for sinus of valsalva aneurysm: 27 year experience with 100 patients. Asian Cardiovasc Annals 2008;16:361-5
- Prian GW, Diethrich EB. Sinus of valsalva abnormalities:a specific differentiation between aneurysms of and aneurysms involving the sinuses of valsalva. Vasc Surg 1973;7:155-64.
- Chu SH et al. Ruptured aneurysms of the sinus of valsalva in oriental patients. J Thorac Cardiovasc Surg 1990;99:288-98
- Choudary SK et al. Aneurysm of sinus of valsalva aneurysm dissecting into interventricular septum. Ann Thorac Surg 1998;65:735-40
- Shah RP et al. A ten-year review of ruptured sinus of valsalva: clinico-pathological and echo-doppler features. Singapore Med J 2001;42:473-6
- Feldman DN, Roman MJ. Aneurysms of the sinus of valsalva. Cardiology 2006;106:73-81
- Cullen S et al. Transcatheter closure of a ruptured aneurysm of the sinus of valsalva. Br Heart J 1994;71:479–80
- Zhao S et al. Transcatheter occlusion of the ruptured sinus of valsalva aneurysm with an amplatzer duct occluder. Inter J Cardiol 2008;129:81-5
- Arora R et al. Transcatheter closure of ruptured sinus of valsalva aneurysm. J Interven Cardiol 2004;17:53-8
- www.CTSnet.org
Abbreviations
| Abbreviation | Term |
|---|---|
| AF | Atrial fibrillation |
| AI /AR | Aortic Insufficiency/ regurgitation |
| AoArch | Aortic arch |
| AS | Aortic stenosis |
| AscAo | Ascending aorta |
| ASD | Atrial septal defect |
| AV | Aortic Valve |
| AVN | Atrioventricualr node |
| BAV | Bicuspid aortic valve |
| CBF | Coronary blood flow |
| Ch | Chamber |
| CHB | Complete heart block |
| CW | Continous wave Doppler |
| IVS | Interventricular septum |
| L | Left |
| LAX | Long axis view |
| LSOVA | Left sinus of Valsalva Aneurysm |
| LV | Left ventricle |
| LVOT | Left ventricular outflow tract |
| ME | Midesophageal view |
| mPA | Main pulmonary artery |
| MR | Mitral Regurgitation |
| MV | Mitral valve |
| NSOVA | Non coronary sinus of Valsalva aneurysm |
| R | Right |
| RA | Right atrium |
| RCC | Right coronary cusp |
| RSOVA | Right sinus of Valsalva aneurysm |
| RV | Right ventricle |
| RVOT | Right ventricular outflow tract |
| RVSP | Right ventricular systolic pressure |
| PA | Pulmonary artery |
| PASP | Pulmonary artery systolic pressure |
| PDA | Patent ductus arteriosus |
| PHT | Pressure half time |
| PV | Pulmonary valve |
| PW | Pulse wave Doppler |
| SAX | Short axis view |
| TG | Transgastric view |
| UE | Upper esophageal view |
| VSD | Ventricular septal defect |
| VT | Ventricular tachycardia |
| VTI | Velocity time integral |