
TEE Colour Doppler
Page Content

Introduction
Two and three-dimensional echocardiography forms the basis of assessing cardiac structure and function. The application of colour Doppler imaging is routinely performed over cardiac valves, vascular and other pathological structures to assess blood flow direction and velocity. This aids the confirmation of pathological diagnoses and quantifies the severity of these lesions.
Module aims
This module demonstrates which structures should be viewed using colour Doppler during the standard 2D examination. Each of the 20 standard views is accompanied by a rotatable three-dimensional heart model and a `colour compare’ video clip which simultaneously shows the two-dimensional and colour Doppler images of each view. Normal blood flow across or within various parts of the heart is shown.
Performing colour Doppler echocardiography
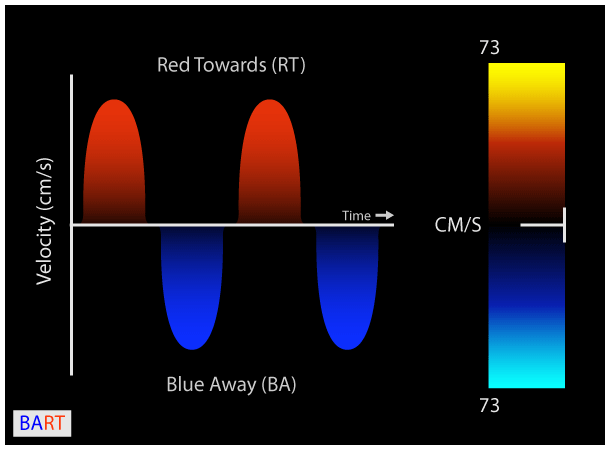
Colour Doppler imaging utilizes multigated Pulse wave Doppler to estimate mean blood flow velocity. Direction of blood flow is displayed using the traditional `BART’ colour scheme where flow away from the probe appears blue (BA) and flow towards the probe appears red (RT). There are 2 colour maps commonly encountered on echo machines:
- Velocity Map - This is based on the `BART’ colour scheme. An enhanced velocity map encodes different blood flow velocities as varying shades of red and blue. The slower the velocity, the darker the shade of red or blue. Similarly, faster velocities are represented in increasingly brighter shades of red and blue (figure 1).
 Figure 1: Colour Doppler Velocity mode.Colour Doppler Velocity mode. Blood flow away from the probe is blue while flow towards is red (BART).
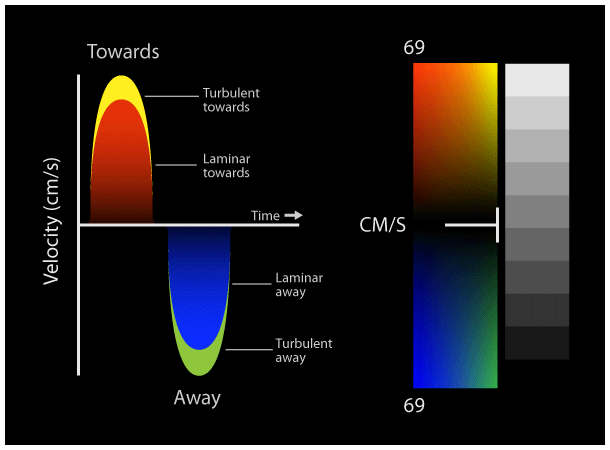
Figure 1: Colour Doppler Velocity mode.Colour Doppler Velocity mode. Blood flow away from the probe is blue while flow towards is red (BART). - Variance Map - This uses the `BART’ scheme but additionally assesses for turbulent flow by representative shades of yellow and green. Turbulence in color Doppler imaging represents the greater variability of blood flow velocity around the mean velocity within each sample volume being measured (figure 2).
 Figure 2: Colour Doppler Variance mode.Colour Doppler Variance mode. Laminar flow is blue or red; turbulent flow is yellow or green.
Figure 2: Colour Doppler Variance mode.Colour Doppler Variance mode. Laminar flow is blue or red; turbulent flow is yellow or green.
The velocity range for each colour map is given by the Nyquist limit (cm/sec). Velocities in excess of the Nyquist limit appear as signal aliasing where red and blue colour flow appear side by side (figure 3). Always set the Nyquist limit scale appropriate to the structure of interest to accurately detect areas of abnormal high velocity flow and quantify the severity of lesions. Inappropriately high scales will miss areas of flow turbulence and underestimate the severity of lesions. Inappropriately low scales will falsely identify areas of flow turbulence and overestimate the severity of lesions.
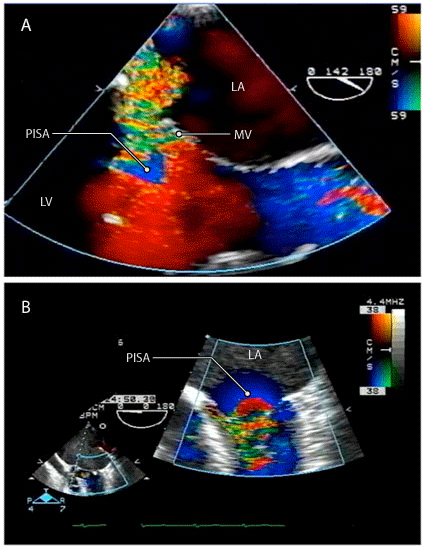
Figure 3: Colour Doppler signal aliasing.
During the application and assessment of colour Doppler images, attention should be paid to the following settings:
- Ensure colour box covers the entire area of interest, for example adequate coverage of the mitral valve and left atrium during the quantification of mitral regurgitation.
- Set the Nyquist limit scale appropriate to the structure of interest. Appropriate scale for valvular and arterial structures is 50-70 cm/sec. Appropriate scale for slower velocity venous structures and the assessment of the interatrial septum is 30-50 cm/sec.
- The Nyquist limit can be crudely altered by changing the color scale. An increase in the pulse repetition frequency increases the Nyquist limit which can be accomplished by reducing the 2D sector depth and choosing a small color box size with a shallower position.
- Minimize aliasing through increasing the Nyquist limit by reducing the color box size and position at a shallower depth which increase the pulse repetition frequency.
Contributors
- Dr. Angela Jerath
Cardiac Anesthesia Fellow
Toronto General Hospital
Department of Anesthesia and Pain Management
- Dr. Annette Vegas
Staff Anesthesiologist
Toronto General Hospital
Department of Anesthesia and Pain Management
- Michael Corrin
Programming & Design
Toronto General Hospital
Department of Anesthesia and Pain Management
