
Spectral Doppler: Left Ventricular Outflow Tract
Obtaining Spectral Doppler Information
- Identify the left ventricular outflow tract (LVOT) in the transgastric views. Each of the following two two-dimensional TEE views can be used:
- Align the pulsed wave (PW) cursor through the aortic valve (AV) (figure 1). Pull the sample volume box into the LVOT until a smooth wave ending with the AV closing click (CC) with minimal spectral broadening is seen (figure 2).
- Note: Visualization of the AV opening click means the cursor is too close to the AV and should be further withdrawn into the LVOT.
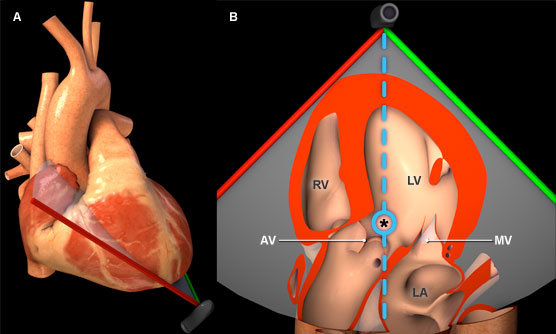
Figure 1: Three-dimensional heart model shown in cross-section to highlight the position of the TEE plane in the deep transgastric view. A) Anterior view of the heart with TEE plane. B) Inferior view of the heart and TEE plane. The blue dotted line represents the orientation of the pulsed wave cursor and the blue circle indicates the position of the sample box in the left ventricular outflow tract. Key: *= Left ventricular outflow tract, AV = Aortic valve, LV = Left ventricle, MV = Mitral valve, RV = Right ventricle.
Features of left ventricular outflow tract spectral Doppler
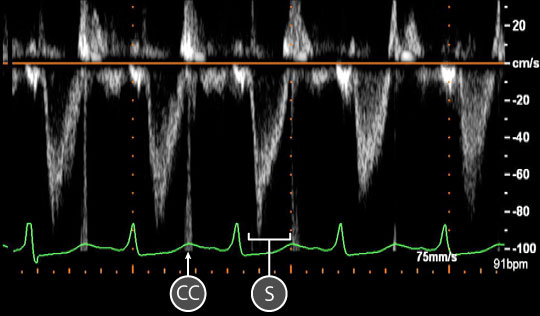
Figure 2: Spectral doppler data acquired for blood flow through the left ventricular outflow tract. A spectral doppler trace shows the relationship between blood velocity and time. The baseline is orange. Key: CC = Aortic valve closing click, S = Systolic wave.
- A single systolic wave is seen below the baseline as blood flow is away from the transducer (figure 2).
- The waveform displays steep acceleration (upstroke) reaching maximum speed during early systole with a lower gradient and a softer deceleration slope.
- The LVOT wave Maximum velocity (VLVOT) is normally in the range of
80 – 100 cm/sec. - The LVOT velocity time integral (VTI) is 15 - 25 cm.
Physiological variation
- Preload dependence
Pathological variation
- Hypertrophic obstructive cardiomyopathy (HOCM)
- Subaortic valvular obstruction