Liver transplant: Living donor right posterior sectionectomy
Donor procedure
00:06 SURGICAL PLANNING
02:47 Mobilization & portal dissection
Case description
- A 54 year old male was worked up as a possible candidate for a living donor liver transplant for his 52 year old wife, who had multi-focal hepatoma.
- Unfortunately, his anatomy precluded both standard right and standard left lobe donation. On his pre-operative imaging, his left lobe was relatively small. As a result, a donor left hepatectomy was not feasible. Similarly, a standard right donor hepatectomy would leave behind too little residual live to be considered "safe."
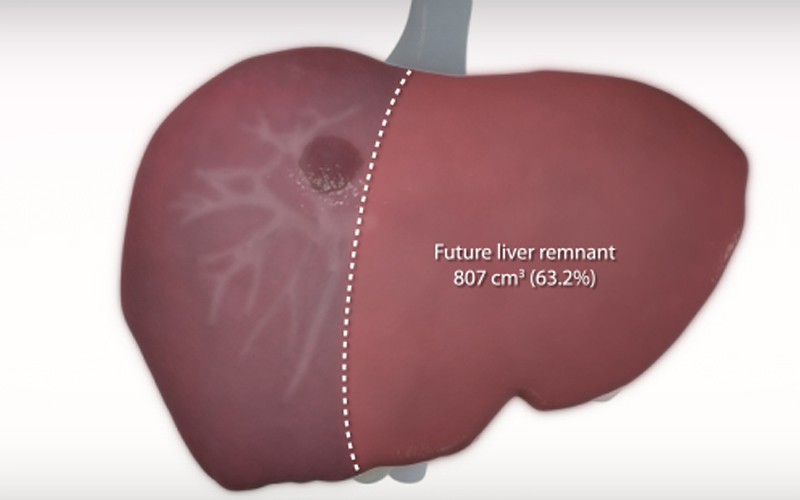
- On the other hand, a donor right posterior sectionectomy (segments 6/7) would yield an adequately-sized graft, while maintaining a safe liver remnant volume for the donor. This resection is complicated due to the fact that the segment 5 arterial inflow arises from the segment 6/7 artery (see arterial phase CT studies, below).
- For the donor posterior sectionectomy, the proposed transection plane will follow the course of the right hepatic vein, sacrificing a segment 5 and a segment 8 hepatic vein branch.
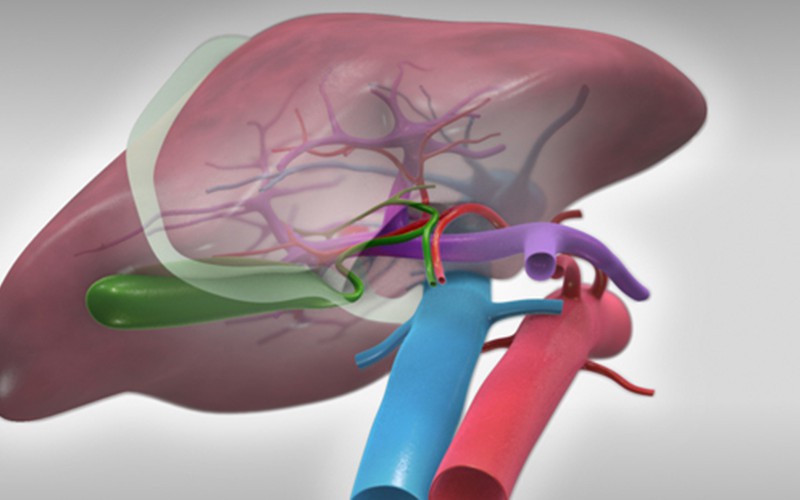
- At the porta, the segment 6 and segment 7 ducts will be divided separately. The segment 6/7 hepatic artery will be divided just after the takeoff of the segment 5 hepatic artery. The right posterior portal vein will be divided.
- As in all donor hepatectomies, an intra-operative cholangiogram will be used to confirm the transection site for the segment 6 and 7 ducts prior to division of the ducts.
- The "hanging liver" maneuver will be used to define the segment 6/7 borders. In this case, the maneuver helps to preserve the segment 5 hepatic artery branch by excluding it from the plane of transection.
CT scans (venous phase)
Click to turn annotations on/off
CT scans (arterial phase)
Click to turn annotations on/off