Total Laparoscopic Hysterectomy
with bilateral salpingo-oophorectomy and staging with omentectomy and sentinel lymph node dissection using ICG imaging
00:05 Surgical planning
02:55 ICG injection and port placement
04:32 Sentinel lymph node dissection
10:33 Bilateral salpingo-oophorectomy
11:53 Hysterectomy
13:18 Omentum biopsy
13:39 Closure
Case Description
- UHN Gynecologic Oncology
- The patient was a 66 year old woman with a high grade endometrial cancer on endometrial biopsy.
- The patient had a previous bilateral tubal ligation.
- A total laparoscopic hysterectomy (TLH) with bilateral salpingo-oophorectomy and sentinel lymph node staging was planned.
- Indocynine Green (ICG) fluorescence dye will be used throughout the procedure to visualize the lymphatics.
- A 25-mg vial of ICG will be reconstituted in 10 mL of sterile water (2.5 mg/mL) and drawn into a spinal needle.
- The ICG dye will then be injected into the patient’s cervix at the 3- and 9-o'clock positions with 0.5 mL of ICG superficially, at 1- to 2-mm depth, and 0.5 mL of ICG at 10-mm depth, for a total dose of 2 mL of ICG.
- ICG will be used to identify the sentinel lymph nodes (SLN) for resection bilaterally.
- The most common area for the sentinel lymph node is the proximal obturator space bilaterally, also known as the lateral paravesical space.
- The main 10mm camera port will be placed in the umbilicus, and a 10mm suprapubic port in the centreline, just above the pubic symphysis.
- Two 5-mm operating ports will be placed in the right, and left lower quadrants.
CT scans
Click to turn annotations on/off
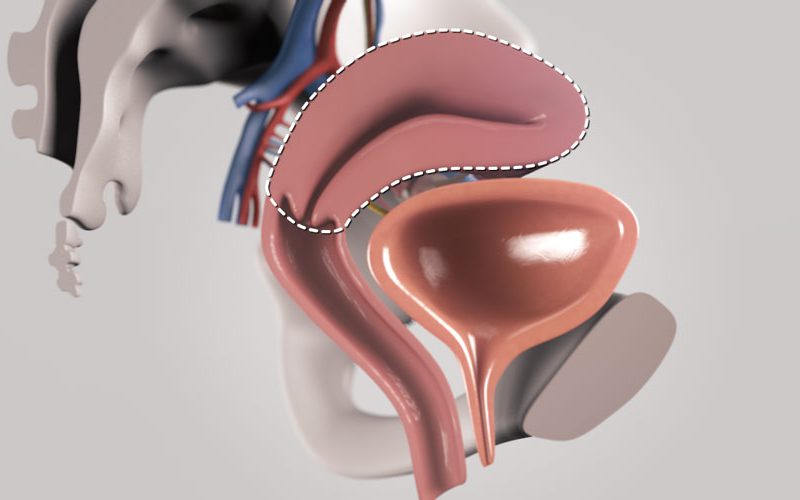
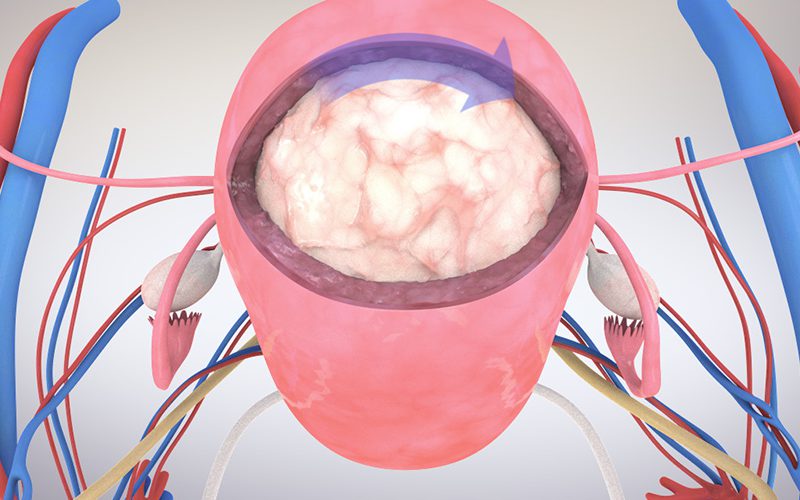
3D anatomy model
Gynecologic surgical anatomy by TVASurg on Sketchfab
Click and drag with LMB to rotate, RMB or MMB to pan. Use mouse scroll wheel to zoom in or out.
References
- Bader, A. A., Winter, R., Haas, J., & Tamussino, K. F. (2007). Where to look for the sentinel lymph node in cervical cancer. American journal of obstetrics and gynecology, 197(6), 678-e1.
- Cormier, B., Rozenholc, A. T., Gotlieb, W., Plante, M., & Giede, C. (2015). Sentinel lymph node procedure in endometrial cancer: a systematic review and proposal for standardization of future research. Gynecologic oncology, 138(2), 478-485.
- Paño, B., Sebastià, C., Ripoll, E., Paredes, P., Salvador, R., Buñesch, L., & Nicolau, C. (2015). Pathways of lymphatic spread in gynecologic malignancies. Radiographics, 35(3), 916-945.
- Persson, J., Geppert, B., Lönnerfors, C., Bollino, M., & Måsbäck, A. (2017). Description of a reproducible anatomically based surgical algorithm for detection of pelvic sentinel lymph nodes in endometrial cancer. Gynecologic oncology, 147(1), 120-125.
- Smith, A. J. B., Fader, A. N., & Tanner, E. J. (2017). Sentinel lymph node assessment in endometrial cancer: a systematic review and meta-analysis. American journal of obstetrics and gynecology, 216(5), 459-476.
- Puntambekar, S., & Manchanda, R. (2018). Surgical pelvic anatomy in gynecologic oncology. International Journal of Gynecology & Obstetrics, 143, 86-92.
- Selçuk, İ., Ersak, B., Tatar, İ., Güngör, T., & Huri, E. (2018). Basic clinical retroperitoneal anatomy for pelvic surgeons. Turkish Journal of Obstetrics and Gynecology, 15(4), 259.
- Kostov, S., Slavchev, S., Dzhenkov, D., Mitev, D., & Yordanov, A. (2020). Avascular Spaces of the Female Pelvis—Clinical Applications in Obstetrics and Gynecology. Journal of Clinical Medicine, 9(5), 1460.