Thoracodorsal artery perforator flap harvest
for head and neck reconstruction procedures
00:10 Surgical planning
03:31 Pre-operative surface markings
04:21 Locating the perforator
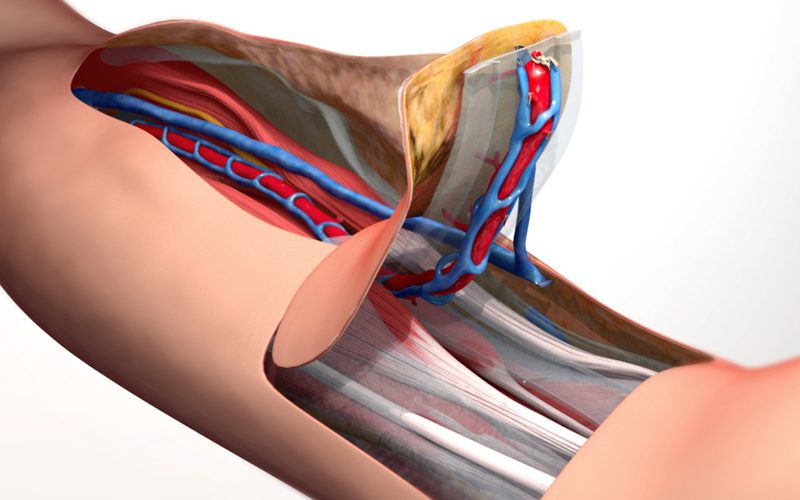
05:45 Dissection of the thoracodorsal pedicle
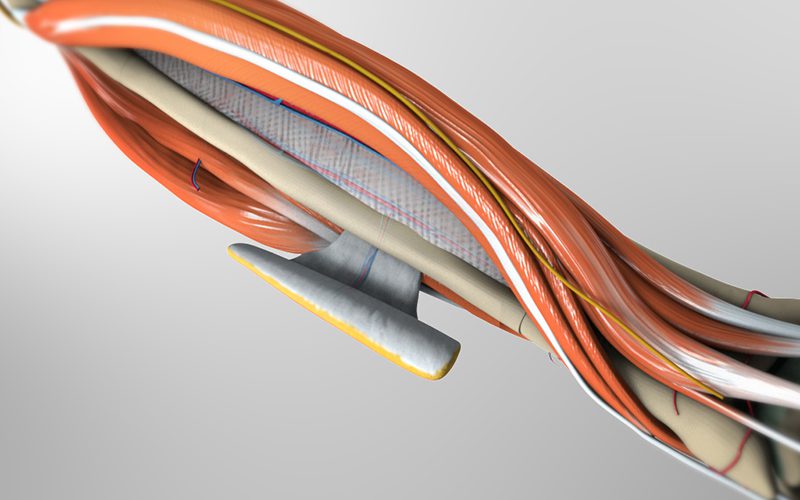
07:22 Intramuscular dissection of the descending branch
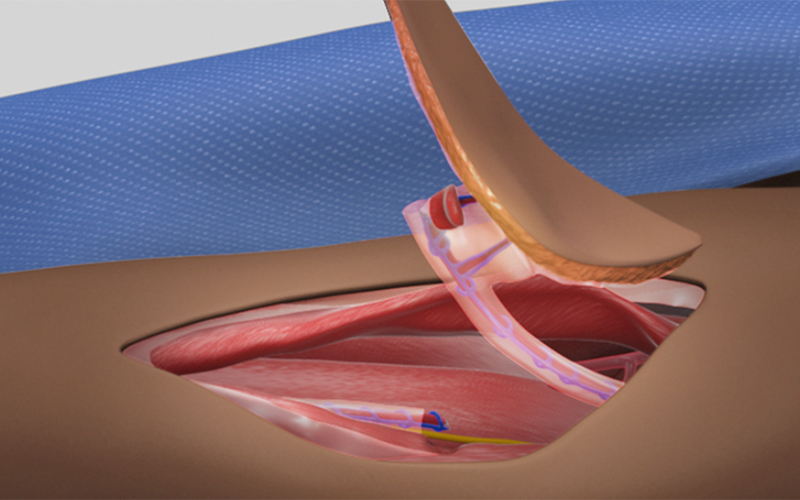
09:15 Flap raising and closure
Case description
- The skin island lies atop the latissimus dorsi muscle, and is supplied by a myocutaneous perforator, arising from the descending branch of the thoracodorsal pedicle.
- The anterior margin of the latissimus dorsi is palpated and marked on the skin surface.
- The perforator is most likely to be found at the two-thirds mark of the muscle border, distal to the axilla.
- During dissection of the muscle, care is taken to identify the axis of the anterior border; this guides subsequent dissection away from the perforator, which is found on the lateral surface of the muscle.
- Skin is carefully dissected away from the lateral surface to identify the perforator, which is usually found within 2cm from the anterior border of the muscle.
- After identifying the perforator, the latissimus dorsi is dissected away from the serratus anterior muscle.
- The serratus branch is identified on the serratus anterior muscle; the descending branch and medial branch are identified on the deep surface of the latissimus dorsi muscle.
- The nerve to latissimus dorsi is identified along the descending branch, and is followed proximally towards the axilla, mobilizing the thoracodorsal pedicle.
- The perforator is followed through the muscle tissue to the descending branch, dividing the overlaying muscle tissue atop the perforator.
- The medial branch, along with the serratus branch are divided between clips.
- The posterior border of the skin island is marked, and traced with electrocautery.
- The skin flap is carefully dissected away from the latissimus dorsi muscle, leaving a safe margin around the perforator.
- The descending branch is divided between clips, distal to the perforator.
- A small cuff of muscle tissue is left on the perforator, for protection as well as acting as an indicator for vessel rotation.
- The pedicle is lifted from the underlying muscle tissue, and divided between clips at the proximal end near the axilla.