Standard right hepatectomy
With portal vein embolization
00:06 Surgical Planning
02:41 Opening & Mobilization
05:45 Right lobe mobilization
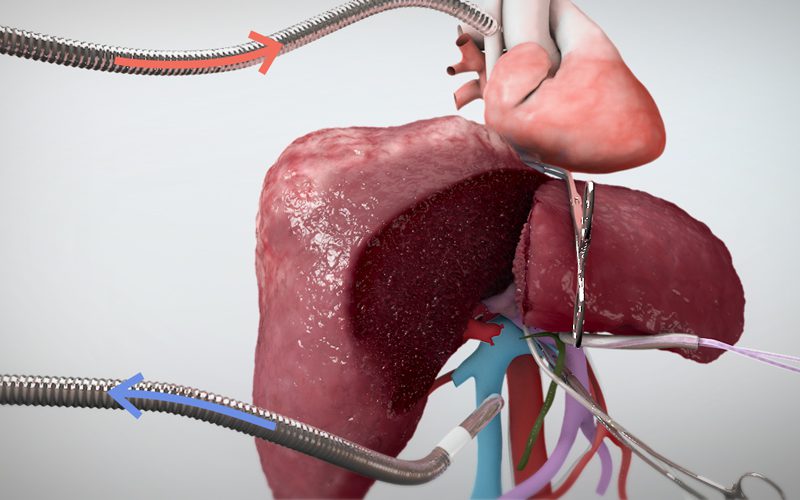
06:29 Parenchymal transection
Case description
- A 57 year old man was diagnosed with hepatitis C, his liver showing mild (Child's A) cirrhosis, with no portal hypertension.
- A 3.2cm hepatocellular carcinoma was found in segments 7 and 8 during surveillance imaging, which involved the right hepatic vein.
- A formal right hepatectomy was suggested as treatment. A portal vein embolization (PVE) procedure was performed to induce hypertrophy in the left lobe, increasing the the future liver remnant (FLR) volume from 513 cm³ (31.4% of total liver volume), to 807cm³ (63.2% of total liver volume).
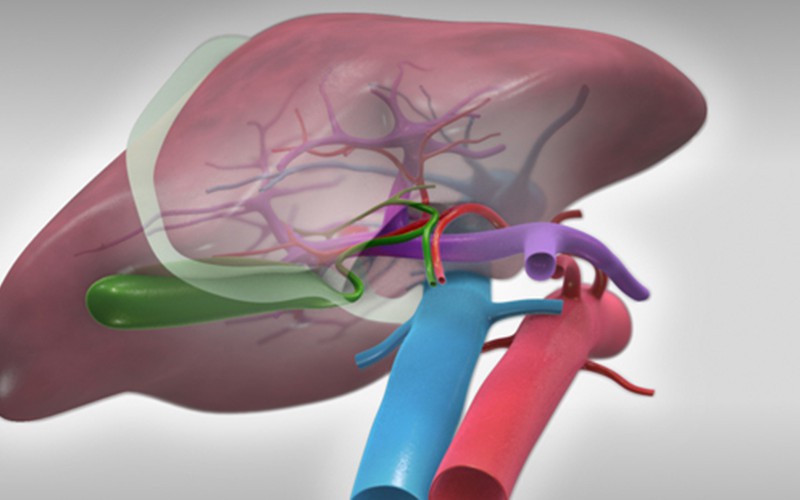
- The anterior and posterior branches of the right hepatic artery, as well as the right portal vein, will be divided at the porta hepatis. The right hepatic duct will remain intact, and will be divided with the intrahepatic biliary plate upon parenchymal transection.
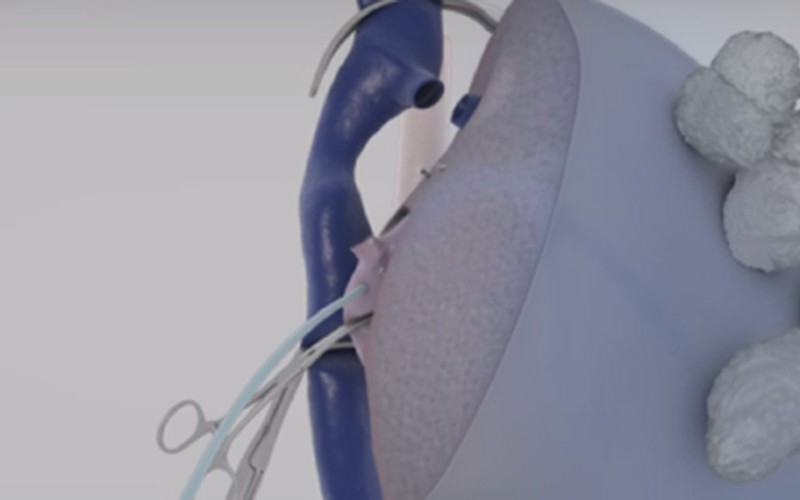
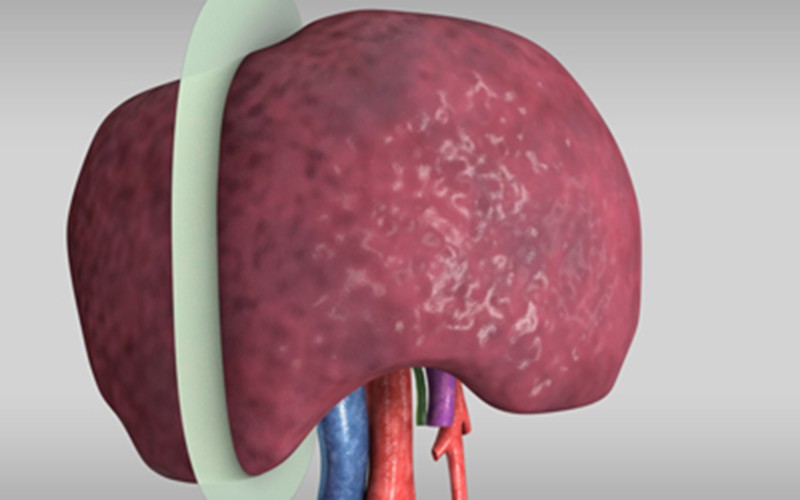
- An umbilical tape will be passed behind the root of the right hepatic vein, passing posterior to the liver, around the divided portal vein and hepatic arteries.
- The tape will act as a 'sling' to indicate the transection plane, which lies to the right of the middle hepatic vein, thus sparing the MHV.
CT scans (pre-PVE, venous phase)
Click to turn annotations on/off
CT scans (post-PVE, venous phase)
Click to turn annotations on/off