radial forearm flap harvest
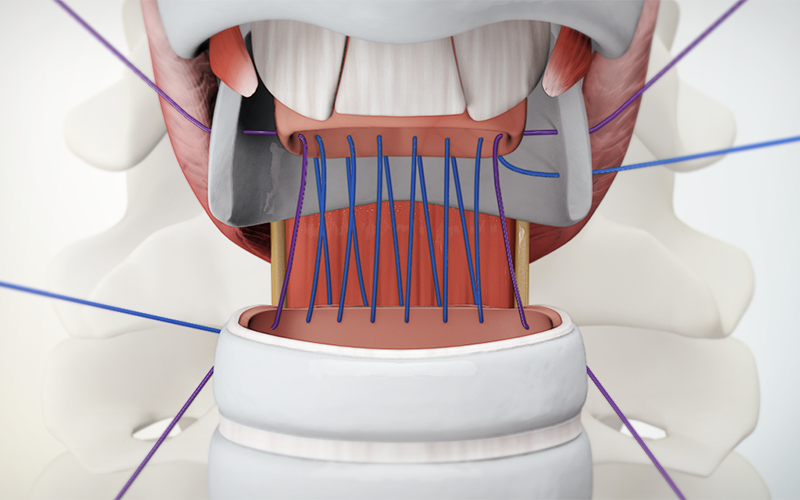
for head and neck reconstruction procedures
00:14 Surgical planning
03:39 Dissection of the cephalic vein
07:27 Dissection of the radial artery pedicle
09:03 Flap raising
CASE DESCRIPTION
- The flap design is marked on the forearm, with a 'S' shape extending from the antecubital fossa to the proximal margin.
- The PL and FCR tendons are dissected at the ulnar border.
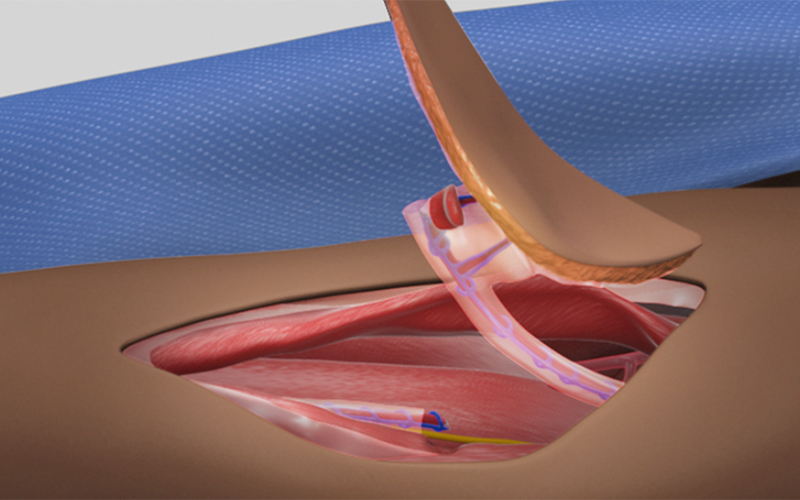
- The cephalic vein is dissected from the proximal margin of the flap to the antecubital fossa.
- At the radial border, cephalic vein branches that drain the skin flap are preserved, while the cephalic vein is divided.
- The radial nerve is identified and preserved.
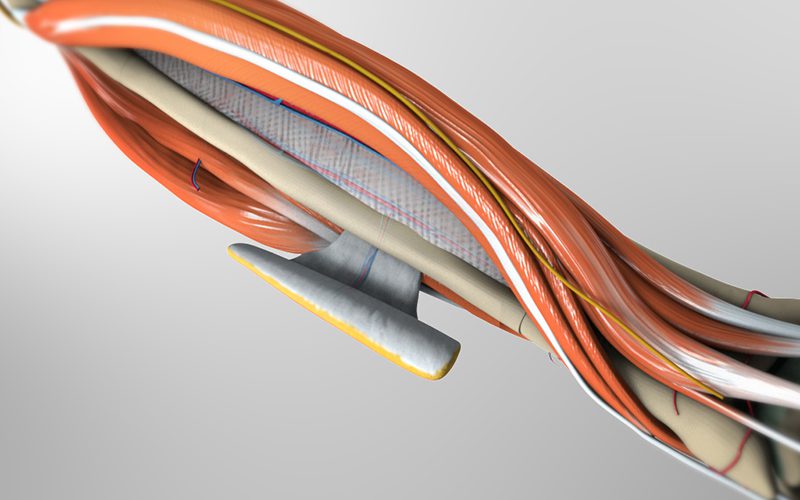
- The BR tendon is identified, and the fascia between the BR muscle and FCR muscle is divided to reveal the radial artery pedicle. The radial artery pedicle is dissected towards the antecubital fossa.
- At the distal margin of the flap, the radial artery pedicle is divided.
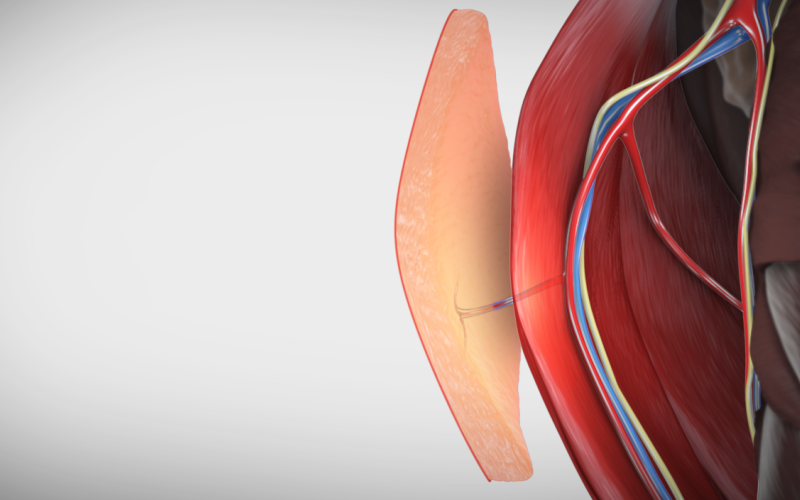
- The skin flap is raised, following a dissection plane above the deep fascia. This ensures that perforator branches from the pedicle supplying the skin flap are preserved.
- The pedicle is mobilized by dividing the inferior and lateral perforators.
- The pedicle and cephalic vein is divided proximally near the antecubital fossa, and the free flap is removed for use in reconstruction.
PEARLS
** Please buy pro to create nested accordion** id="14608"]