Surgical Planning
- In operative hysteroscopy, intrauterine pathologies are visualized, and then removed.
- Operative hysteroscopy can be performed using loop electrosurgical resection, mechanical tissue removal, and mechanical tissue extraction using instruments, such as scissors or a grasper attached to the hysteroscope.
- Large or symptomatic endometrial polyps, or submucosal fibroids that bulge significantly into the uterine cavity, are removed hysteroscopically.
- Cervical preparation can be considered for patients at higher risk of difficult dilation.
- Particular care should be taken to firmly secure the plastic fluid collection bag to the patient.
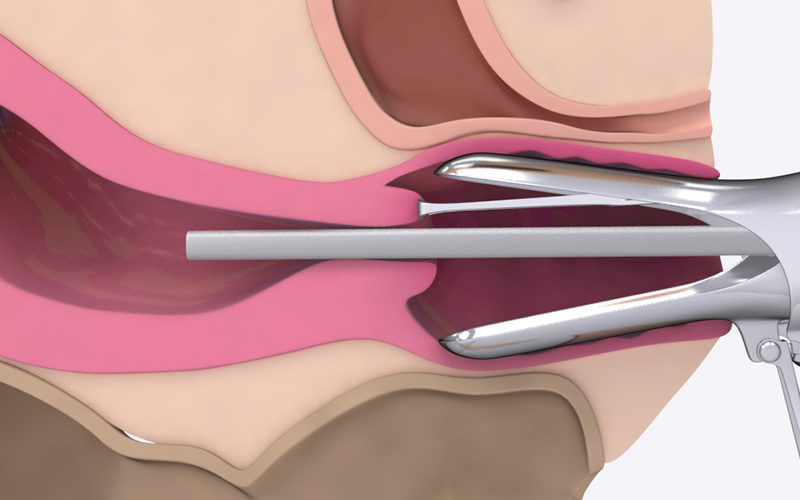
- The cervix is dilated to the appropriate diameter, depending on the size of the hysteroscope.
- The fluid inflow, and outflow can be adjusted, to ensure a clear view of the uterine cavity. This is a dynamic balance that requires continuous re-adjustment throughout the case.
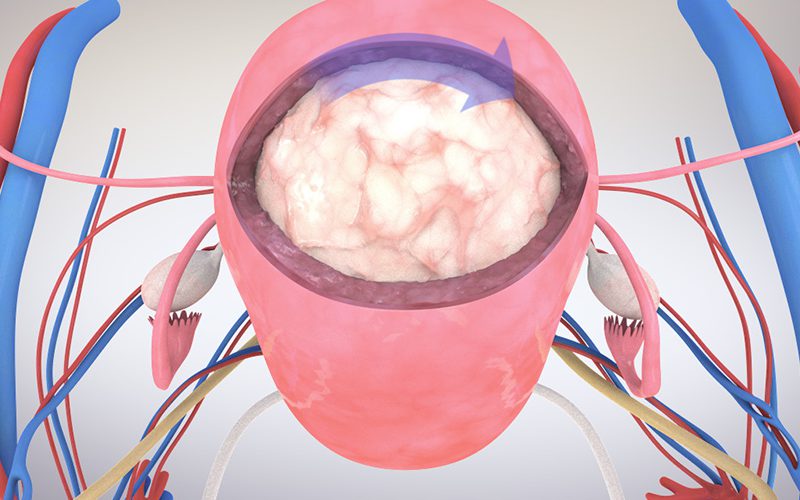
- During resection with an electrosurgical loop, best practice is to move the loop in a cranial to caudal direction. Plan the approach by practicing the intended movements without activating electrosurgical energy.
- In the case of small polyps, the uterine cavity is inspected, and scissors are used to detach the small polyp at the base, and the entire hysteroscope is removed under direct visualization.
- Newer mechanical tissue removal systems can remove larger specimens by using a rotating blade to cut, and simultaneously aspirate the tissue.
- Operative hysteroscopy is a safe and effective option to diagnose and treat intrauterine pathology such as polyps or submucosal fibroids.
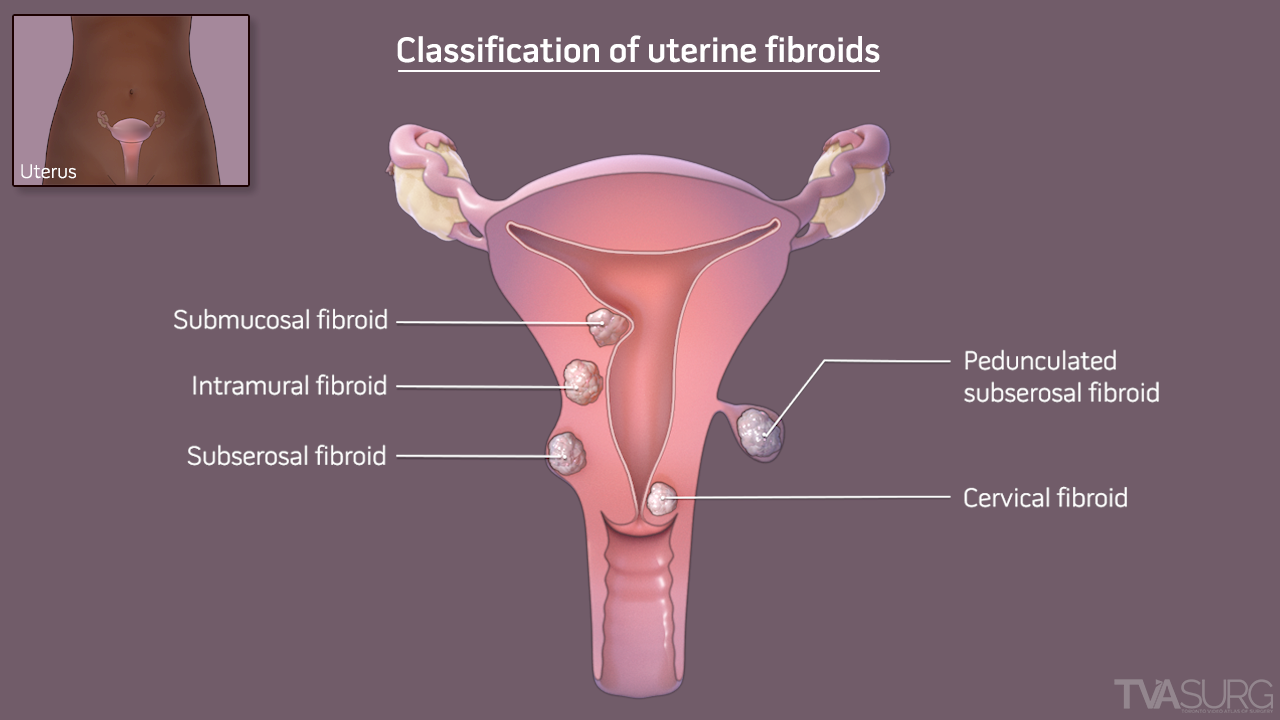
Types of fibroids
- Fibroids can be located within the following locations of the uterus:
- Intramural – within the muscular wall
- Subserosal - on the outer surface
- Pedunculated - on a stalk attached to the exterior surface
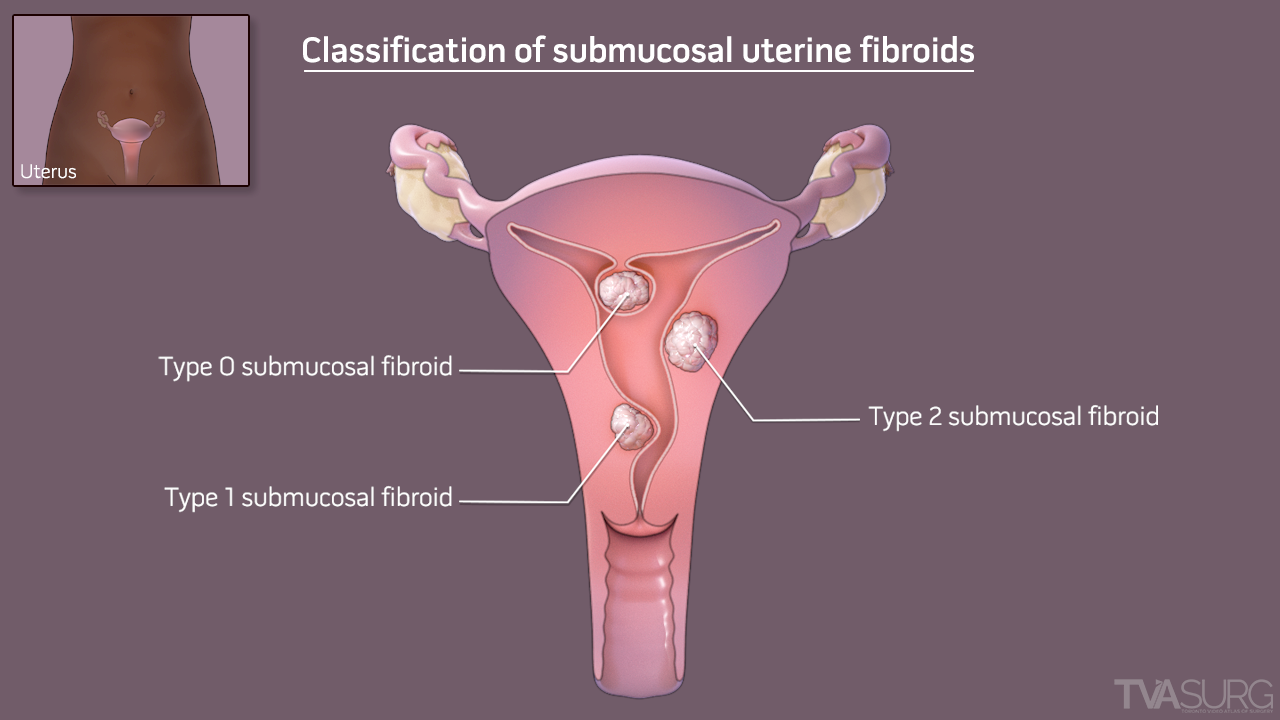
- Submucosal – within the cavity
- Type 0: Pedunculated within the uterine cavity
- Type 1: More than 50% of the fibroid protrudes into the cavity
- Type 2: Less than 50% of the fibroid protrudes into the cavity
- Less commonly, fibroids can arise from the broad ligament, cervix, or vagina