LAPAROSCOPIC ANATOMICAL RESECTION OF SEGMENT 4B AND 8
with skeletonization of bile duct bifurcation and hepatic veins
Conference details
This video was presented by Dr. David Henault at the International Society of Liver Surgeons (ISLS) 2023 Congress of International Advanced HBP Surgery.
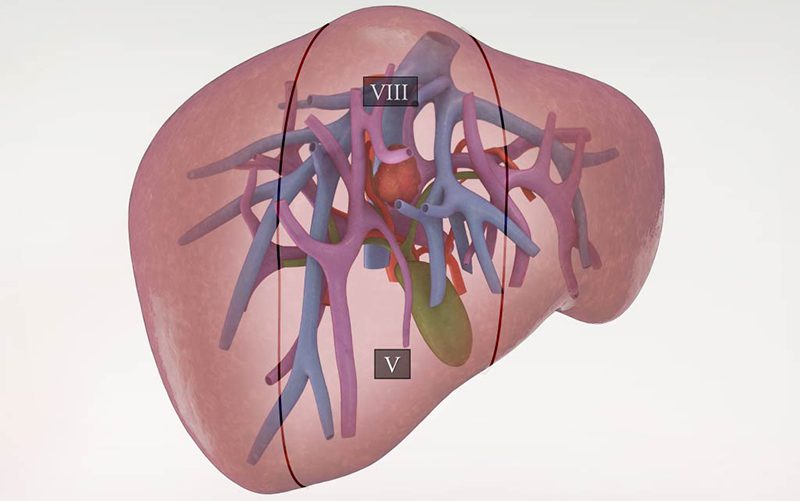
- A 76-year-old woman was diagnosed with right sided T3N1 colorectal adenocarcinoma which was treated with laparoscopic right hemicolectomy. She was diagnosed with two liver metastases in segment 4b (sitting on top of the bile duct bifurcation) and in segment 8, less than one year after removal of her primary tumor.
- This video demonstrates the surgical technique employed to laparoscopically perform the resection of a segment 4b tumor and of a segment 8 tumor in proximity to the right and middle hepatic veins.
- The patient was placed supine with both arms out and in reverse Trendelenburg position.
- The trocars were placed as following: 12 mm supraumbilical, two 12 mm trocars in the right and left subcostal and 5 mm in the epigastrium and right flank. The right liver was fully mobilized with the Harmonic device and the laparoscopic intraoperative ultrasound was used to locate the tumors.
- The cholecystectomy was first performed, and the porta was encircled with an umbilical tape and a chest tube to perform intermittent Pringle maneuvers.
- An anatomical segment 4b resection using the caudal view was performed using the CUSA Clarity dissector. The bile duct bifurcation was identified and skeletonized. The tumor was separated from it by pushing up the Gleason capsule. Vascular and biliary branches originating from the bifurcation were transected with vascular staplers. ICG green fluorescence was used to improve visualisation.
- An anatomical segment 8 resection was performed second using the same technique.
- A root to periphery approach was performed on the middle hepatic vein until the segment 8 vein was skeletonized and transected. The mass was resected after complete skeletonization of the middle and right hepatic vein.
- The estimated blood loss was approximately 200 mL and the patient had a length of stay of 4 days without complication during or after hospitalisation.