Anatomy and Pathology
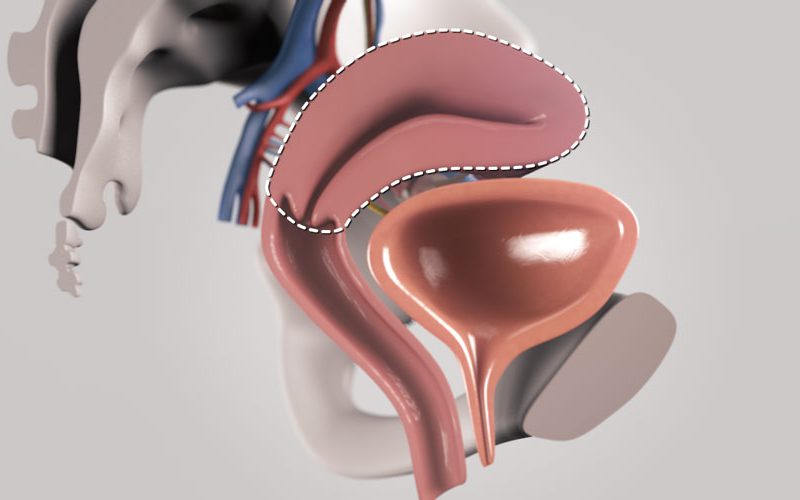
- Uterine fibroids are benign, hormone sensitive tumours that arise from the smooth muscle layer of the uterus.
- Fibroids are asymptomatic up to 50% of the time. However, fibroids may cause heavy menstrual bleeding, bulk symptoms, and/or infertility depending on their size and location.
- The patient is a 32 year-old female with a 10 cm fundal intramural uterine fibroid, causing significant bulk symptoms and heavy menstrual bleeding.
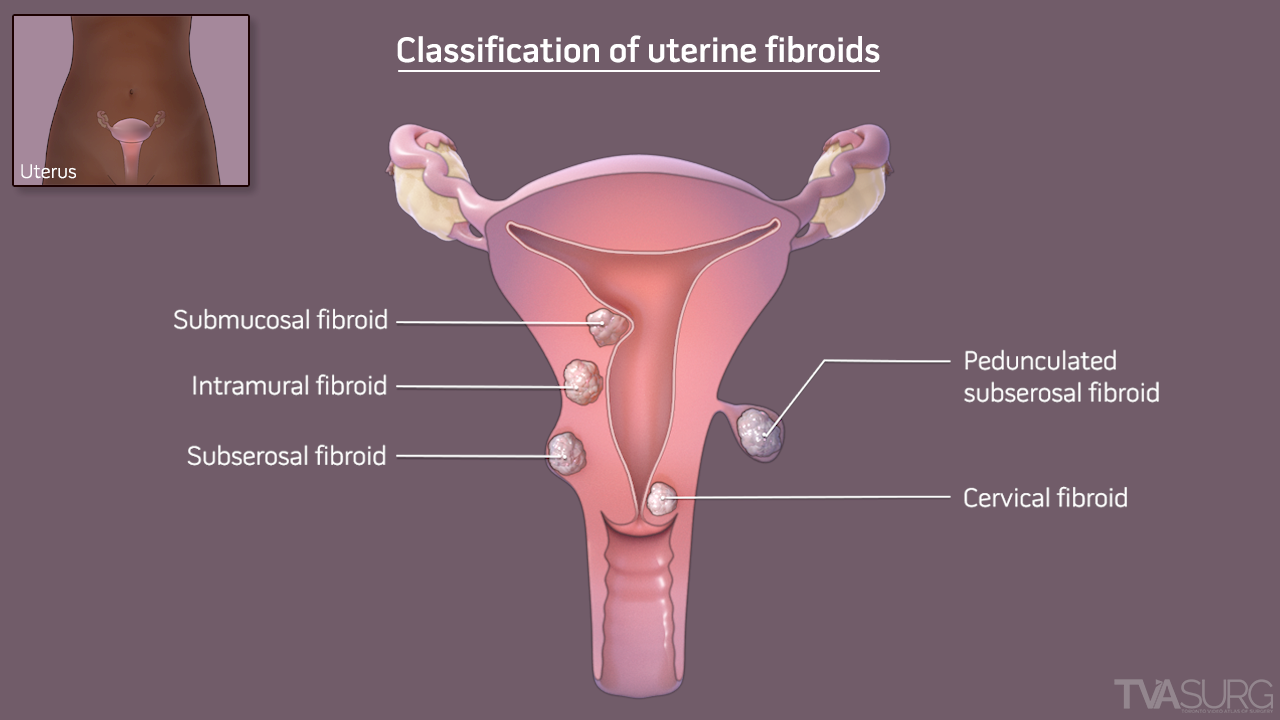
- Fibroids can be located within the following locations of the uterus:
- Intramural – within the muscular wall
- Subserosal - on the outer surface
- Pedunculated - on a stalk attached to the exterior surface
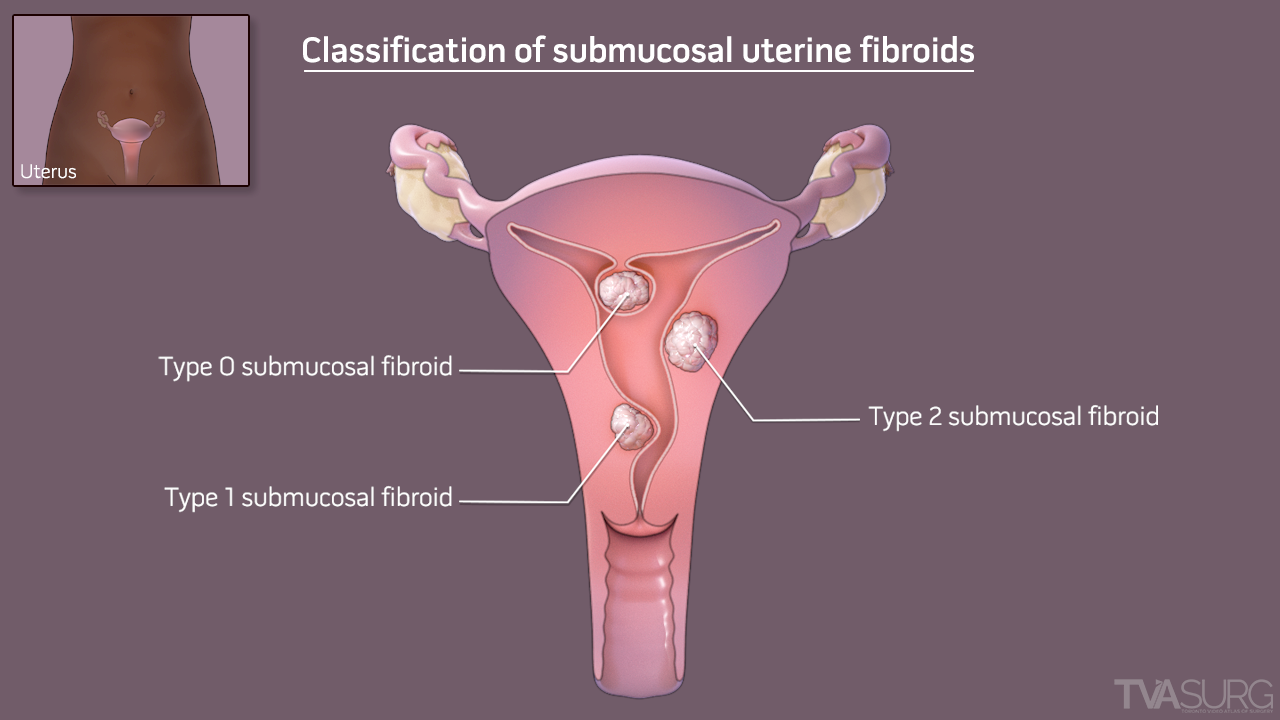
- Submucosal – within the cavity
- Type 0: Pedunculated within the uterine cavity
- Type 1: More than 50% of the fibroid protrudes into the cavity
- Type 2: Less than 50% of the fibroid protrudes into the cavity
- Less commonly, fibroids can arise from the broad ligament, cervix, or vagina
Surgical Planning
- A laparoscopic myomectomy was planned for this case.
- Myomectomy is the surgical removal of a fibroid from the uterus.
- Myomectomy may be approached hysteroscopically for submucosal fibroids that distort the uterine cavity.
- Intramural, subserosal, and pedunculated fibroids may be removed either via laparotomy or laparoscopy.
- Laparoscopic myomectomy may be considered in cases where there is adequate uterine mobility and sufficient space for visualization and surgical access. It is typically limited to less than 5 to 10 fibroids on imaging, that are less than 10 cm in size.
- Familiarity of the surgical team and comfort of the surgeon with the procedure are keys to a successful laparoscopic myomectomy.
- Pre-operative planning is essential when considering a myomectomy.
- It is crucial to optimize a patient’s hemoglobin prior to elective myomectomy. In addition to iron supplementation, various medications can be started to reduce or eliminate menstrual bleeding.
- Medications that shrink fibroids may also facilitate surgery and allow for a minimally invasive surgical approach.
- Imaging with ultrasound or MRI is necessary to map the number, size and location of fibroids. A sonohysterogram may be useful to delineate a submucosal component.
- The patient was pre-treated with a 3-month course of Leuprolide Acetate (Lupron), in order to induce amenorrhea and shrink the fibroid prior to surgery.
Management to Minimize Blood Loss
- To mitigate the risk of excessive blood loss, a number of medical and surgical techniques can be employed at the time of surgery.
- Medical options:
- Intravenous tranexamic acid
- Rectal misoprostol
- Intramyometrial dilute vasopressin
- Surgical techniques to decrease blood flow to the uterus also to reduce blood loss and blood transfusion:
- A tourniquet can be secured around the uterus or fibroid, to reduce bleeding during its excision.
- Temporary or permanent clipping of the uterine arteries bilaterally can be performed prior to hysterotomy.
Surgical Procedure
- The patient is positioned in dorsal lithotomy with legs in yellow-fin stirrups, in steep Trendelenburg.
- To allow sufficient room to operate, the camera is placed cephalad to the umbilicus. One accessory port is placed on the right lower quadrant, and two accessory ports are on the left.
- A transverse uterine incision is made down to the level of the fibroid.
- The fibroid plane will be dissected circumferentially to allow for enucleation, and the fibroid will be removed.
- A 0 barbed delayed absorbable suture is used to re-approximate the myometrial defect in layers.
- The myometrial defect can be closed with a running non-barbed suture or simple interrupted sutures.
- The specimen is extracted using an eleven-blade scalpel to morcellate the fibroid with a “c-incision” technique.
- The specimen retrieval can also be made of laparoscopic in-bag morcellation.
Post-operative Care
- Most patients may be safely discharged on the day of surgery following an uncomplicated laparoscopic myomectomy.
- Unless the fibroid is pedunculated, patients are generally advised to undergo caesarean section in any subsequent pregnancies, to minimize the risk of uterine scar dehiscence and uterine rupture.