FIBULA OSTEOCUTANEOUS flap harvest
for head and neck reconstruction procedures
00:13 Surgical planning
02:55 Exposure & flap marking
05:26 Mobilize flap
07:49 Osteotomies
08:59 Distal pedicle
09:24 Flap raising
11:28 Proximal pedicle
12:23 Flap harvest
Pearls & Pitfalls
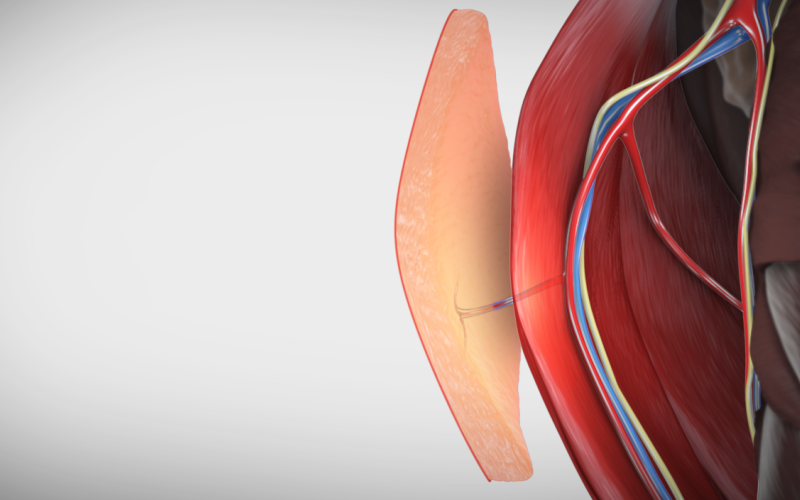
- Osteotomies will be performed 6 cm from the head of the fibula superiorly, to 6 cm from the lateral malleolus of the ankle inferiorly. Right-angle dissectors should be inserted posterior to the fibula to protect the vascular pedicle during distal and proximal osteotomy.
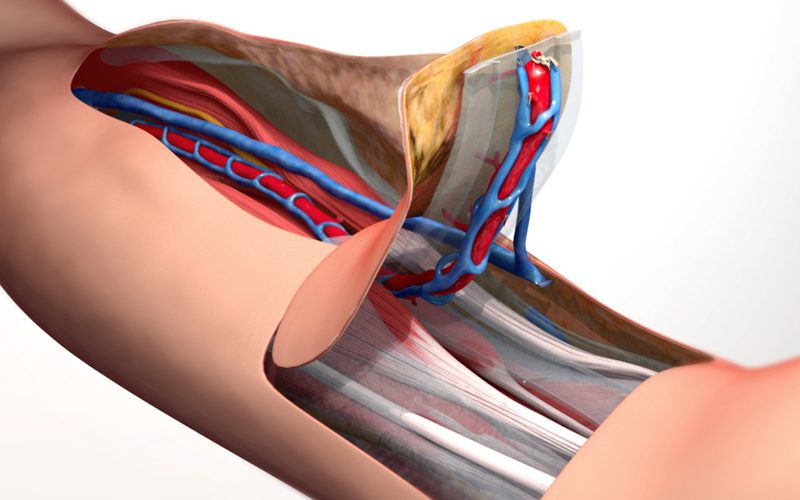
- Up to 18 cm of bone is available for the osteocutaneous flap, for this case, 10 cm will be harvested, as well as a 3 cm by 5 cm skin paddle island, and a 10 cm length of vascular pedicle, including the peroneal artery and 2 vena comitantes.
- The vascular pedicle is released from the fibula after completing the harvest to provide pedicle length for microvascular anastomosis in the neck.
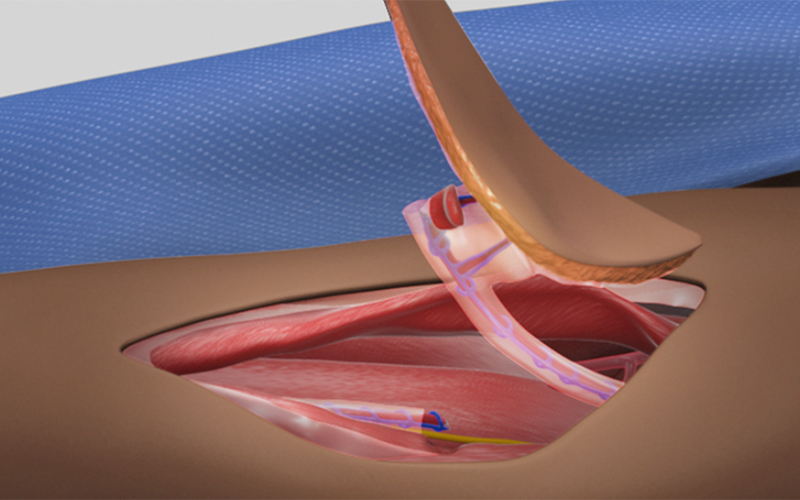
- In this case, the septum containing the perforators to the skin was released from the fibula to allow rotation of the skin island, if this degree of mobilization is not required the septum can be left intact to prevent tethering or injury of the perforator to the skin island.
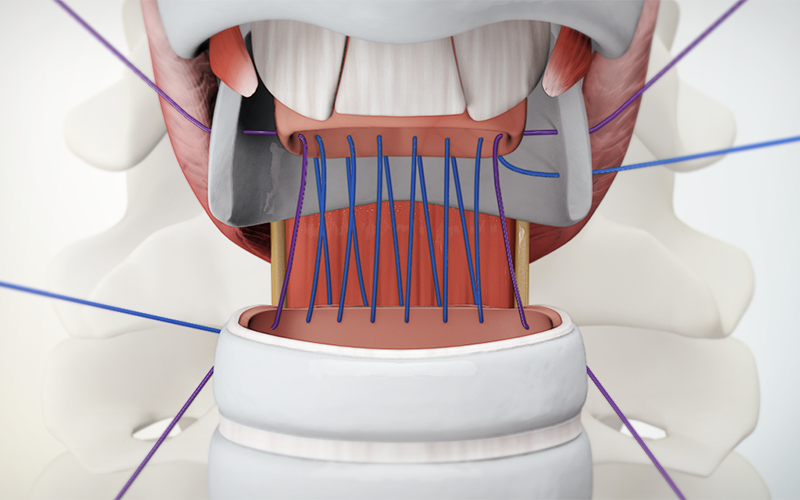
- In this video the final dissection and separation of the proximal artery and venae comitantes of the vascular pedicle are performed while the tourniquet is inflated. This approach is appropriate for experienced flap surgeons. For less experienced surgeons, proximal peroneal pedicle dissection and mobilization should be done after the tourniquet is deflated, in order to prevent prolonged ischemia times should the pedicle be injured during this dissection.
- Patients with significant varices in the leg may have very large medial perforating veins making dissection technically difficult and tedious. The use of an Esmarch bandage to exsanguinate the leg prior to tourniquet inflation can assist with technical difficulty of this dissection.