Ex-vivo liver I/VI/VII segmentectomy with en bloc caval resection and right nephrectomy
Presented by Dr. Ian McGilvray
00:05 PRE-OPERATIVE IMAGING
01:35 OPENING INCISION & INTRA-OPERATIVE TEE
02:29 MOBILIZATION OF INFERIOR VENA CAVA & PORTAL DISSECTION
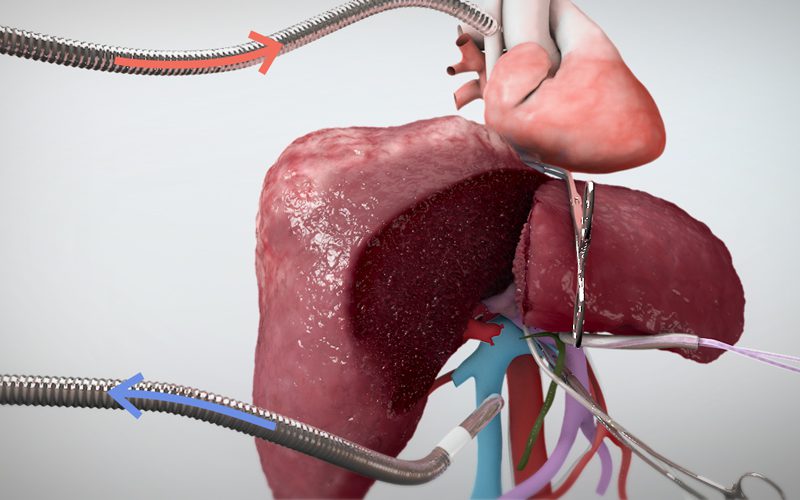
03:14 VASCULAR EXCLUSION & SPECIMEN REMOVAL
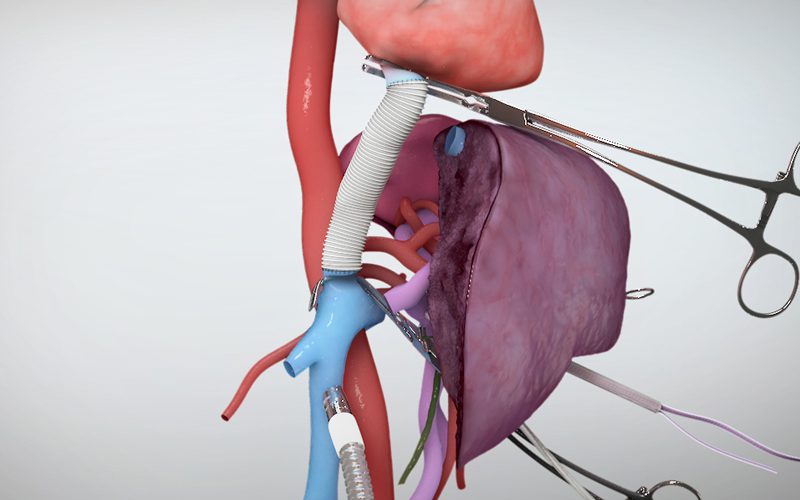
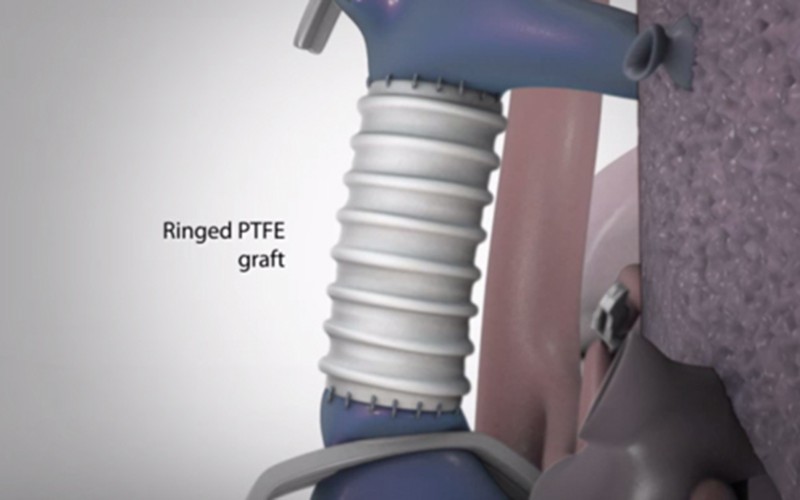
04:18 CONSTRUCTION OF CAVAL GRAFT & TEMPORARY PORTO-CAVAL SHUNT
05:01 BACKBENCH: REMOVAL OF BLOOD CLOT
06:10 LIVER RE-IMPLANTATION & VASCULAR RECONSTRUCTION
This video was presented at the 2015 Canadian Surgical Forum, and was awarded 'Best of Show' in the video abstract category.
Tumors involving the retrohepatic vena cava pose significant technical challenges, particularly when liver outflow is involved. Retroperitoneal sarcomas require multidisciplinary evaluation and discussion but resectability is a surgical decision based on the patient's anatomy, as well as on surgical techniques and available resources. Innovative surgical techniques can allow resection even in complex cases that would otherwise remain unresectable by standard criteria.
In this video we present the case of a leiomyosarcoma arising from the inferior vena cava, extending into the right atrium and involving the right hepatic vein in a young 43 year old patient. Surgical planning was modified at the time of surgery when intraoperative ultrasound revealed bland thrombosis of the middle and left hepatic veins, an acute development leading to a Budd-Chiari syndrome. We used an ex-vivo technique to perform en bloc liver resection (segments 1, 6, 7), right nephrectomy, adrenalectomy and atrio-caval resection and reconstruction with a ringed PTFE graft. After removal of the liver and specimen, a temporary porto-caval shunt was created while the liver was prepared on the backbench. Liver auto-transplantation permitted safe and accurate reconstruction of the middle and left hepatic veins, while protecting the liver parenchyma from ischemic damage.
The patient remains well and cancer free more than 8 months from the date of surgery. This complex case illustrates the feasibility of combining liver transplantation and resectional techniques to expand therapeutic options in the oncology setting.