Caesarean Section in Patients with an Elevated BMI
00:29 Surgical Planning
03:54 C-section Preparation & Patient Position
06:14 Abdominal Entry
08:27 Delivery of Infant
09:59 Uterine Closure
11:50 Abdominal Closure
CASE DESCRIPTION
- The patient is a 30 year old G2P1 with a body mass index of 70 and one prior Caesarean section. The patient elected to have a repeat Caesarean section for delivery.
- Following a supra-umbilical transverse incision, the subcutaneous tissue, rectus fascia and peritoneum are divided.
- In patients with an elevated BMI, the excess adipose tissue may stretch the rectus fascia and displace the rectus abdominis muscles laterally. A slightly upward curved transverse incision is made on the rectus fascia, keeping a safe distance from the rectus abdominis muscle and the inferior epigastric arteries.
- An abdominal surgical retractor is placed to maximize exposure of the uterus.
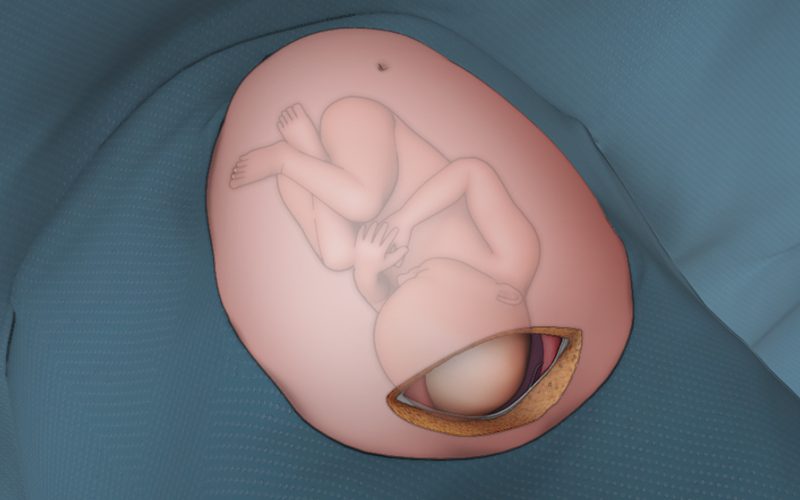
- A transverse incision is made in the lower uterine segment. The infant’s head is flexed and gently elevated towards the uterine incision. With lateral support to maintain the infant in caudal-cranial axis, fundal pressure is applied to facilitate delivery.
- The uterine closure is performed in two layers. The first layer is approximated using a locked continuous suture. The second layer uses an imbricating method, burying the first layer of closure.
- The peritoneum and the rectus fascia are closed. The subcutaneous tissue is closed in layers, followed by skin closure.
- A negative pressure wound therapy system is used to facilitate healing and minimize wound complications.