ABDOMINAL MYOMECTOMY
Through Maylard incision
00:11 Surgical planning
03:15 Entry and exposure
06:33 Abdominal myomectomy
11:16 Abdominal closing
Case description
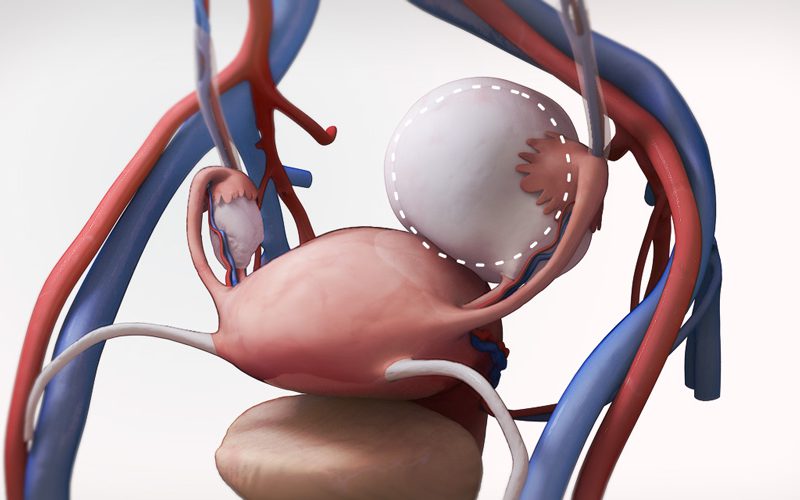
- The patient was a 32-year-old G1P1 with fundal subserosal (FIGO type 7) fibroid, measuring 17cm.
- A Maylard incision is planned, which increases exposure and access to the pelvic sidewalls, compared to a Pfannenstiel incision, while allowing for a transverse skin incision.
- The incision involves dividing the rectus muscles, as well as the inferior epigastric arteries, located at the postero-lateral border of the rectus muscles.
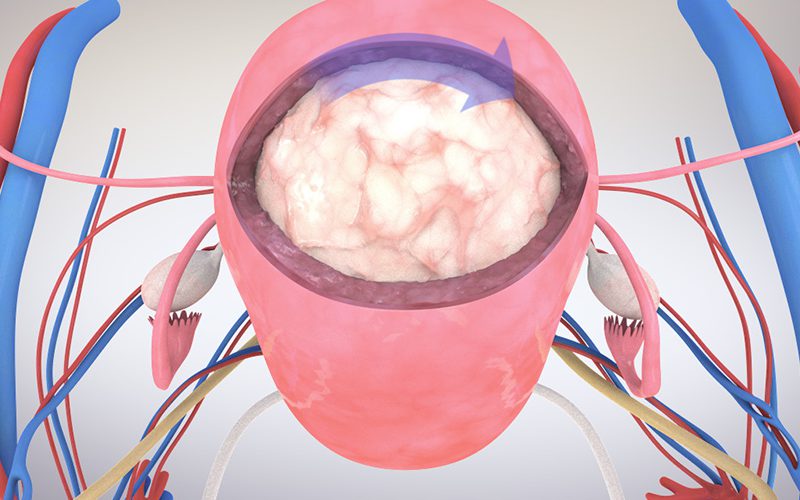
- The uterus was exteriorized from the abdominal cavity, along with the fibroid.
- A Penrose drain was passed through the broad ligament windows and secured anteriorly to temporarily occlude blood flow through the uterine arteries to minimize bleeding.
- Dilute vasopressin was injected as an acute vasoconstrictive agent, at the proposed site of excising the fibroid.
- The fibroid was carefully removed and the myometrial defect was re-approximated in layers.
- The uterine serosa was re-approximated using a baseball or herringbone suture technique.
- The peritoneum is closed, along with the fascia and skin. The rectus muscles will heal spontaneously without sutures.
Contradictions to Maylard incision
- Patients with with significant peripheral vascular disease, as the inferior epigastrics are important as collateral circulation to lower limbs in this population.
Additional information
FIGO type 1-7 fibroid classifications
Hapugoda S, Uterine leiomyoma (fibroid) classification system (illustration). Case study, Radiopaedia.org