Labour progress

The stages of labour include:
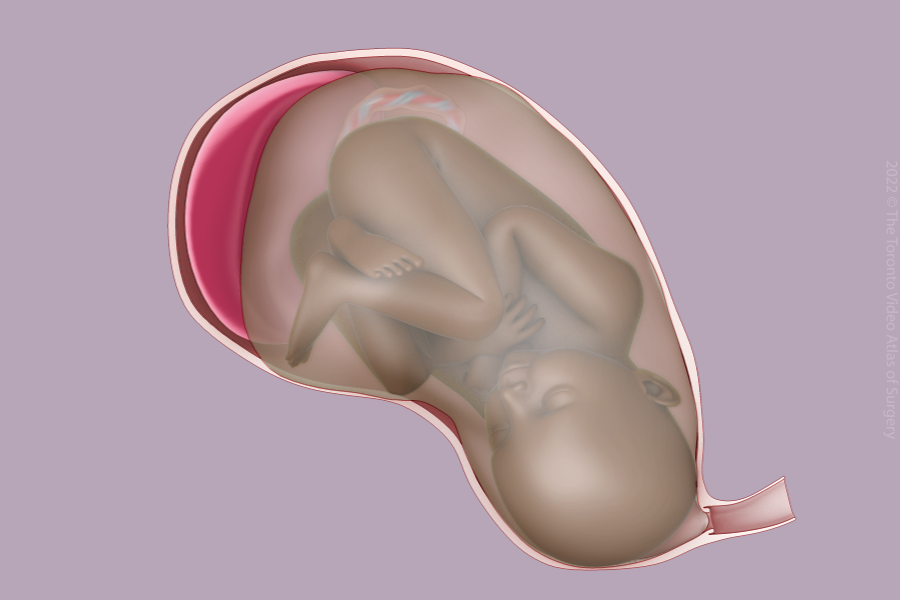
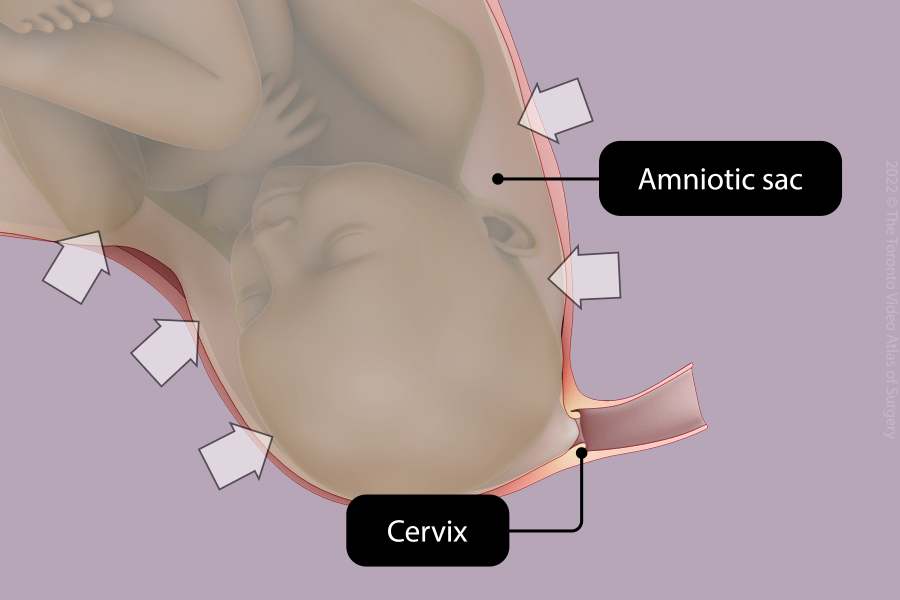
- 1st Stage: Thinning and opening of the cervix
- 2nd Stage: Birth of the baby
- 3rd Stage: Delivery of the placenta
- 4th Stage: Immediate postpartum period
The frequency of contractions and the baby’s heart rate will be monitored throughout labour. The baby’s heart rate is a reflection of how the baby is reacting to labour.
Regular strong contractions are required to thin and open the cervix. These contractions may occur spontaneously or require help from medications (i.e., oxytocin, misoprostol).
If the water does not break spontaneously, your water may be gently broken by your care provider to strengthen the contractions.
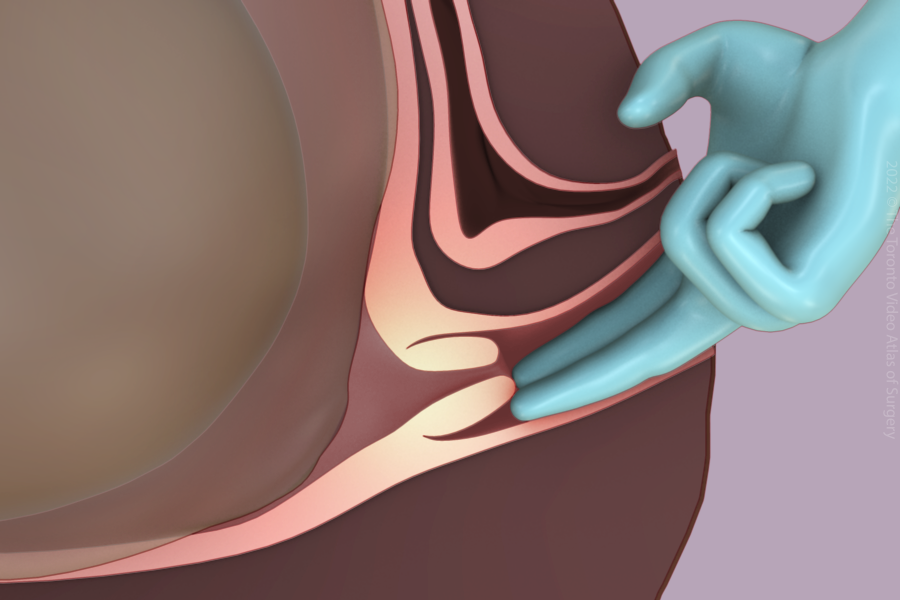
The team will check your cervix throughout labour by inserting two fingers into the vagina. As labour progresses, the cervix should open until it is fully dilated (10 cm).
If you have an epidural, your bladder may need to be emptied with a catheter (small tube).
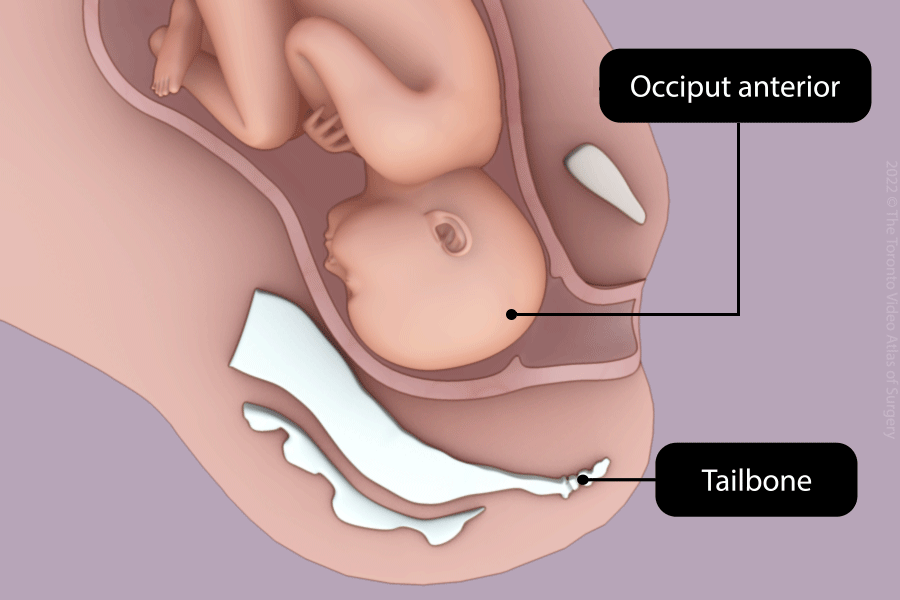
Once the cervix is fully dilated, the position and the station are assessed to determine when you should start pushing.
Ideally the baby is positioned facing your back. If the baby is not in this position, your care provider may use their hand to rotate the baby.
You will start pushing once the head is close to coming out. Sometimes this means waiting for your contractions to bring the head down.

There are many pushing positions - none are better than others. The most common position is semi-seated with legs pulled back.
Most patients push 3-4 times for 10 seconds each with every contraction. Many first time parents push for at least an hour.
If the baby doesn’t deliver or tolerate pushing, your care provider may recommend an episiotomy, vacuum, forceps, or Cesarean delivery.
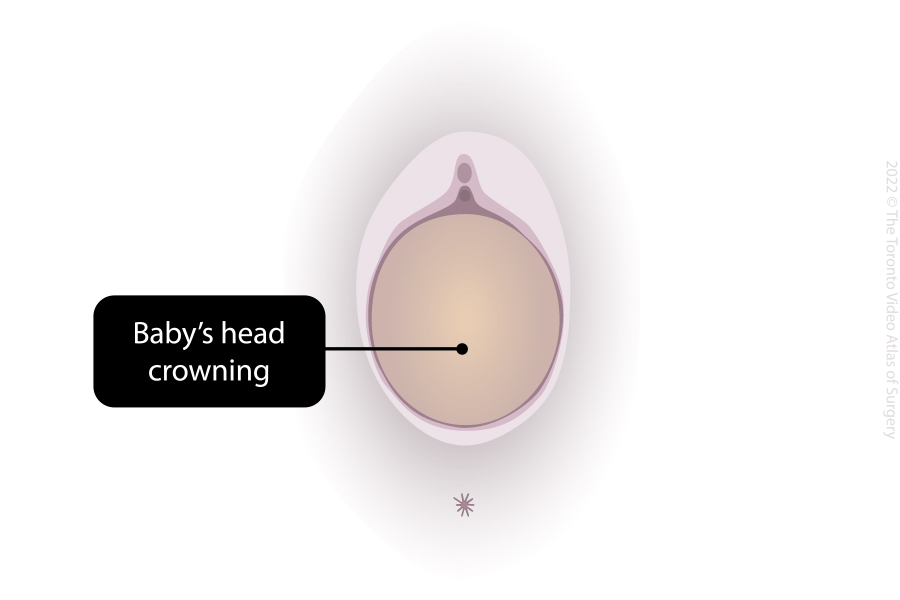
The vaginal skin will stretch as the baby delivers. Your care provider is there to minimize tearing. You may be asked to stop pushing to allow the baby to come out more slowly. Sometimes an episiotomy will be recommended.

At delivery, the baby is handed directly to you to promote skin-to-skin. Delayed cord clamping can take place at this time. If there are any concerns, the baby will be given to the care team. Generally, the baby stays with you the entire time.
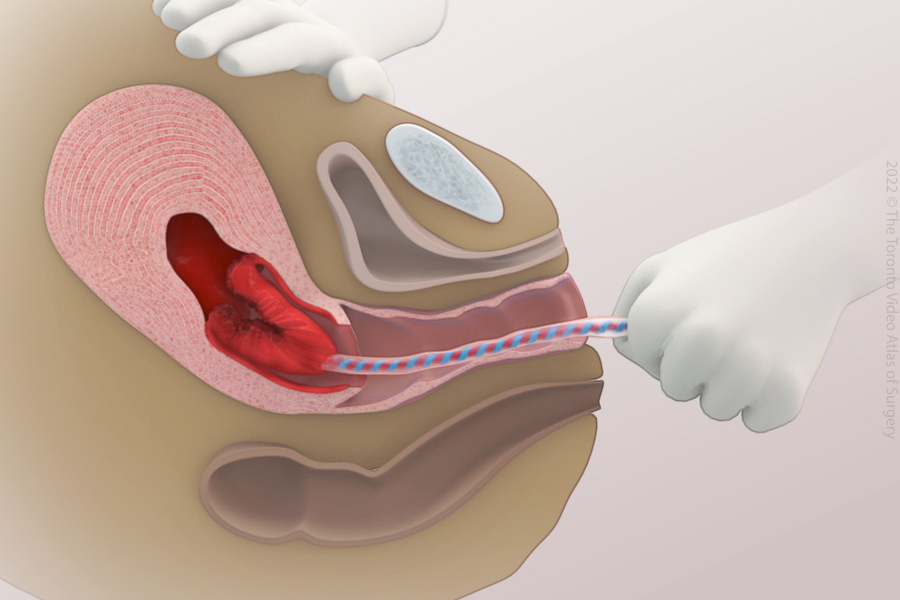
Once the cord has been clamped and cut, the team will wait for the placenta to deliver.
Oxytocin and gently pulling on the cord have been shown to speed up placenta delivery and minimize bleeding.
If the placenta does not separate, your care provider may need to gently remove it with their hands or surgical instruments.
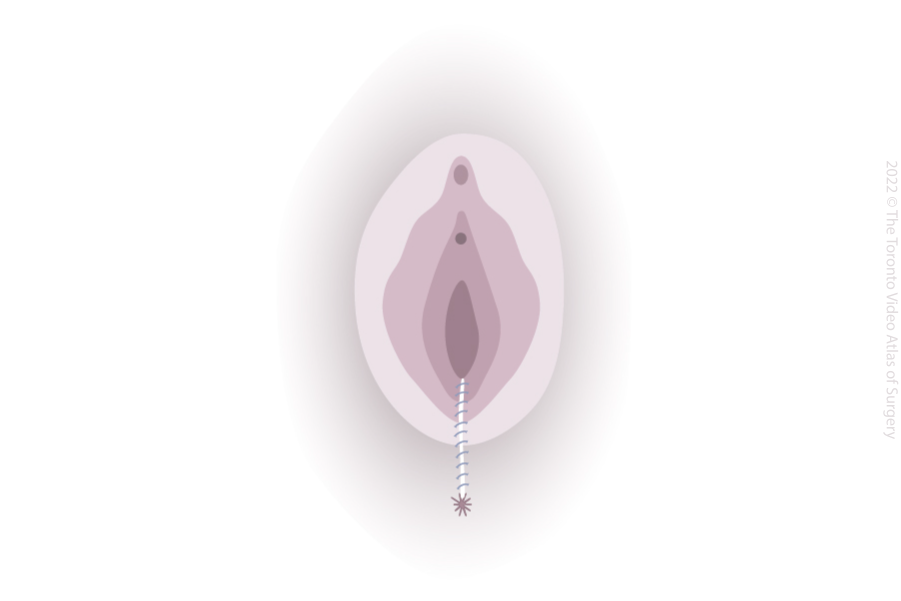
Your care team will carefully inspect your vagina and anus for tears.
These tears are repaired using dissolvable stitches.
Pain is controlled with either your epidural, laughing gas, or extra freezing.
During this time, your care team will watch carefully for any ongoing bleeding.